ACRAL LICK GRANULOMA
- At a glance
- WHAT DOES IT LOOK LIKE?
- WHAT ELSE LOOKS LIKE THIS?
- HOW DO I DIAGNOSE IT?
- HOW DO I MANAGE IT?
- COMMENTS
AT A GLANCE
- A self-induced thickening and possible ulcer of the skin secondary to the trauma of chronic licking
- Multiple etiologies may lead to the desire to lick
- Uncommon in dogs, rare in cats





WHAT DOES IT LOOK LIKE?
- Variably sized, thickened, alopecic, erythematous and very firm plaques usually over a distal extremity such as the carpal/metacarpal (61% of cases) or tarsal/metatarsal region (Pathologic Image Library - Figure 1).
- Lesions are usually solitary.
- Lesions are often ulcerated centrally and may discharge a serous to purulent exudate (Pathologic Image Library - Figure 2).
- Patients may continue to lick obsessively at lesions throughout the exam if not restrained
- More common in large breed dogs with predisposed breeds including Doberman pinschers (Pathologic Image Library - Figure 3), Labrador retrievers, Golden retrievers, Weimeraners, Great Danes, Boxers, Irish Setters and German shepherd dogs
WHAT ELSE LOOKS LIKE THIS?
- Neoplasia (squamous cell carcinoma, mast cell tumor, cutaneous lymphoma)
- Deep bacterial pyoderma
- Fungal granuloma
- Traumatic injuries
HOW DO I DIAGNOSE IT?
- The clinical appearance is highly suggestive
- Skin scrapings to rule out demodicosis
- Surface cytology to screen for bacterial or fungal involvement
- Deep tissue culture to guide antibiotic selection
- If necessary, histopathology to rule out other differentials, particularly deep mycoses or neoplasia
- Radiograph of the affected limb to identify underlying arthropathy
HOW DO I MANAGE IT?
- The vast majority of lesions have a deep bacterial pyoderma component associated which requires extended courses of antibiotics to resolve
- Antibiotics should ideally be chosen based on deep tissue cultures and given for 2 weeks beyond resolution of the infectious component, which may take several months
- The cause of the licking behavior must be identified and resolved to prevent on-going self-trauma
- Barrier preventatives such as E-collars or bandages may be useful to minimize continued self-trauma in the initial stages
- Agents to deter licking such as capsaicin cream, Bitter Apple, HEET and anti-lick bandages are helpful in some cases.
- 50% of cases found to be licking due to idiopathic or behavioral causes, though other triggers should be investigated and resolved if possible
- Other potential triggers include allergies (flea, food environmental), demodicosis, neuropathy, arthritis, prior trauma and underlying osteopathy; treatment and resolution of these triggers, if present, may prevent recurrence
- In the absence of an organic trigger a psychogenic trigger or stress should be sought such as:
- Long periods of confinement or boredom
- Death in the family
- New addition to the family (baby, dog, cat etc)
- Children having moved away
- Environmental enrichment and removal or reduction of identified stressors is beneficial where possible
- Psychoactive drugs may be necessary in some cases and are especially effective in conjunction with behavior modification
- Fluoxetine (1 mg/kg q 24hrs) or clomipramine (1-3 mg/kg q 24 hrs) are reported to be the most effective psychoactive drugs while others that have been used successfully include:
- Amitriptyline 1-3 mg/kg PO every 24 hrs
- Hydroxyzine 2 mg/kg PO every 8 hrs
- Diazepam 0.2 mg/kg PO every 12 hrs
- Naltrexone 2 mg/kg PO every 24 hrs
- Hydrocodone 0.25 mg/kg PO every 8 hrs
- A combination of 8 ml of Synotic with 3 ml of Banamine applied to lesions twice daily was shown to be effective for some cases
- Particularly refractory cases may benefit from surgical removal either via excision, or laser ablation, though this is typically used as a last resort as the response is variable
COMMENTS
- Idiopathic or behaviorally-induced lesions are often solitary, while acral lick granulomas induced by other triggers may have additional dermatologic signs or histories suggestive of the underlying etiology
- Psychoactive medications used in treatment trials may need to be administered for 4-5 weeks to assess efficacy
- Prognosis for cure is guarded
- Virga V. Behavioral dermatology. Vet Clin North Am Small Anim Pract. 33 (2003): 231-251.
- Miller W, et al. Muller and Kirk's Small Animal Dermatology, 7th ed. Canine Psychogenic Dermatoses. Elsevier, 2013.
abscess
A discrete swelling containing purulent material, typically in the subcutis

Perianal abscess in a dog
alopecia
Absence of hair from areas where it is normally present; may be due to folliculitis, abnormal follicle cycling, or self-trauma

Extensive alopecia secondary to cutaneous epitheliotropic lymphoma
alopecia (“moth-eaten”)
well-circumscribed, circular, patchy to coalescing alopecia, often associated with folliculitis

“Moth-eaten” alopecia secondary to superficial bacterial folliculitis




hemorrhagic bullae
Blood-filled elevation of epidermis, >1cm

Interdigital hemorrhagic bulla in a dog with deep pyoderma and furunculosis
comedo
dilated hair follicle filled with keratin, sebum
Comedones on the ventral abdomen of a dog with hypercortisolism
crust
Dried exudate and keratinous debris on skin surface

Multifocal crusts due to pemphigus foliaceus



epidermal collarettes
Circular scale or crust with erythema, associated with folliculitis or ruptured pustules or vesicles

Epidermal collarettes in a dog with Staphylococcus superficial bacterial folliculitis
erosion
Defect in epidermis that does not penetrate basement membrane. Histopathology may be needed to differentiate from ulcer.

Erosions in a dog with vasculitis
erythema
Red appearance of skin due to inflammation, capillary congestion

Erythema in a dog with cutaneous drug eruption
eschar
Thick crust often related to necrosis, trauma, or thermal/chemical burn

Eschar from physical trauma
excoriation
Erosions and/or ulcerations due to self-trauma

Excoriations in a cat with atopic dermatitis
fissure
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Fissures of the footpads in a dog with superficial necrolytic dermatitis
fistula
Ulcer on skin surface that originates from and is contiguous with tracts extending into deeper, typically subcutaneous tissues

Perianal fistulas in a dog
follicular casts
Accumulation of scale adherent to hair shaft

Follicular casts surrounding hairs from a dog with hypothyroidism
hyperkeratosis
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Idiopathic hyperkeratosis of the nasal planum (left) and footpads (right)
hyperpigmentation
Increased melanin in skin, often secondary to inflammation

Inflammatory lesions (left) resulting in post-inflammatory hyperpigmentation (right)

hypotrichosis
Lack of hair due to genetic factors or defects in embryogenesis.

Congenital hypotrichosis in chocolate Labrador puppies.

lichenification
Thickening of the epidermis, often due to chronic inflammation resulting in exaggerated texture

Lichenification of skin in a dog with chronic atopic dermatitis and Malassezia dermatitis
macule
Flat lesion associated with color change <1cm

Pigmented macule (left) Erythematous macule (right)
melanosis
Increased melanin in skin, may be secondary to inflammation.

Post inflammatory hyperpigmentation of this dog’s thigh
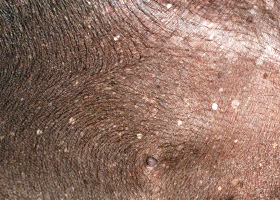
miliary
Multifocal, papular, crusting dermatitis; a descriptive term, not a diagnosis

Miliary dermatitis in a flea allergic cat
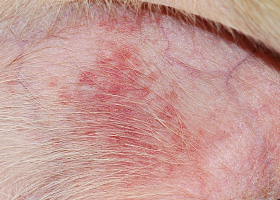
morbiliform
A erythematous, macular, papular rash; the erythematous macules are typically 2-10 mm in diameter with coalescence to form larger lesions in some areas

Morbiliform eruptions in a dog with a cutaneous drug reaction

onychodystrophy
Abnormal nail morphology due to nail bed infection, inflammation, or trauma; may include: Onychogryphosis, Onychomadesis, Onychorrhexis, Onychoschizia

Onychodystrophy in dog with chronic allergies
onychogryphosis
Abnormal claw curvature; secondary to nail bed inflammation or trauma

Onychogryphosis in a dog with symmetric lupoid onychodystrophy
onychomadesis
Claw sloughing due to nail bed inflammation or trauma

Onychomadesis in a dog with symmetric lupoid onychodystrophy
onychorrhexis
Claw fragmentation due to nail bed inflammation or trauma

Onychorrhexis in a dog with symmetric lupoid onychodystrophy
onychoschizia
Claw splitting due to nail bed inflammation or trauma

Onychoschizia in a dog with symmetric lupoid onychodystrophy

patch
Flat lesion associated with color change >1cm

Hypopigmented patch (left), erythematous patch (right)
petechiae
Small erythematous or violaceous lesions due to dermal bleeding

Petechiae in a dog with cutaneous vasculitis
phlebectasia
Venous dilation; most commonly associated with hypercortisolism

Phlebectasia and cutaneous atrophy due to hypercortisolism in a dog
plaques
Flat-topped elevation >1cm formed of coalescing papules or dermal infiltration

Plaques in a cat with cutaneous lymphoma
pustule
Raised epidermal infiltration of pus

Pustules on the abdomen of a dog with superficial staphylococcal pyoderma.
scale
Accumulation of loose fragments of stratum corneum

Loose, large scales due to ichthyosis in a Golden Retriever
scar
Fibrous tissue replacing damaged cutaneous and/or subcutaneous tissues

Scarring (right) following the healing of an ulcer (left) in a dog with sterile nodular dermatitis
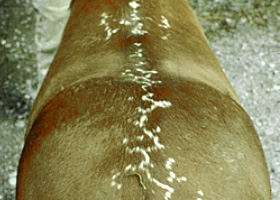
serpiginous
Undulating, serpentine (snake-like) arrangement of lesions

Serpiginous urticarial lesions on a horse
telangiectasia
Permanent enlargement of vessels resulting in a red or violet lesion (rare)

Telangiectasia in a dog with angiomatosis
ulcer
A defect in epidermis that penetrates the basement membrane. Histopathology may be needed to differentiate from an erosion.

Ulcerations of the skin of a dog with vasculitis.
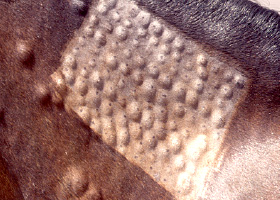
urticaria
Wheals (steep-walled, circumscribed elevation in the skin due to edema ) due to hypersensitivity reaction

Urticaria in a horse
vesicle
Fluid-filled elevation of epidermis, <1cm

Vesicles and bullae on ear pinna due to bullous pemphigoid
wheal
Steep-walled, circumscribed elevation in the skin due to edema
Wheals associated with intradermal allergy testing in a horse