ALLERGIC DERMATOSES : ATOPIC DERMATITIS - CANINE
- AT A GLANCE
- WHAT DOES IT LOOK LIKE?
- WHAT ELSE LOOKS LIKE THIS?
- HOW DO I DIAGNOSE IT?
- HOW DO I MANAGE IT?
- COMMENTS
What Is It?
- A genetically predisposed inflammatory and pruritic allergic skin disease with characteristic clinical features associated with IgE antibodies most commonly directed against environmental allergens
- Mode of inheritance is unknown; environmental factors may be important in the development of the disease
- Defects in the skin barrier may play an important role in allergen exposure
- Allergens are absorbed through the skin and captured by cutaneous Langerhans cells which present them to T-helper 2 lymphocytes in the dermis. This results in release of inflammatory mediators, cytokines that increase allergen-specific IgE as well as cytokines that cause direct neuronal stimulation and itch
- (Link to www.itchcycle.com MOA videos)







What Does It Look Like?
- Can occur in any breed of dog but is more commonly diagnosed in the terrier breeds (West Highland White, Cairn, fox terrier, etc), golden retriever and setters
- Mean age of onset is 1-3 years but may begin as early as 6 months of age
- May be seasonal or year round
- Estimate that 8% of dogs have AD
- The major clinic feature is pruritic behavior – scratching, rubbing, licking, chewing
- The pruritus responds to treatment with glucocorticoids
- Primary lesions are rare and most of the clinical signs are secondary to self trauma
- Most commonly affected areas are the periocular, perioral, caudal carpus and tarsus, inner pinnae and axillae
- Secondary skin infections with Staphylococcus and Malassezia are common
What Else Looks Like This?
- Other allergic and pruritic dermatoses
- Food allergy (cutaneous adverse reactions to food)
- Flea bite hypersensitivity
- Sarcoptic mange
- Pruritic pyoderma
- Malassezia infections
How Do I Diagnose It?
- The diagnosis of AD is made by exclusion of other causes of pruritic dermatitis
- Intradermal testing or measurement of serum allergen-specific IgE is used to select allergens used for hyposensitization (see below), not to make the diagnosis


How Do I Treat It?
- JAK Inhibitor
- A different class of medication that specifically targets the cytokines involved in itch and inflammation associated with allergic skin conditons with minimal negative impact on immune function
- Monoclonal antibody
- Caninized monoclonal antibody (mAb) targeting interleukin-31 (IL-31): aids in the reduction of clinical signs associated with atopic dermatitis in dogs. IL-31 has been shown to induce pruritus in dogs in laboratory studies
- Corticosteroids
- Provide rapid relief from itching and control of inflammation
-
- prednisone (prednisolone) – 0.25-0.5 mg/kg PO SID for 3-7 days to start and then tapered to the lowest effective dose
-
- Avoid repeated injections of long acting or repository corticosteroids
-
- Safe annual dose of prednisone
-
-
- Body Weight (kg) X 30 = mg prednisone / year
-
-
- Antihistamines
- None are approved for use in veterinary medicine
- Evidence-based medicine fails to show that they provide benefit in the treatment of AD
- Cyclosporine
- 5mg/kg PO SID x 30 then decrease frequency
- Fatty acids
- Oral and topical supplementation with ω-3 FAs may help in moderating inflammation and improving the skin barrier
- Topical therapy
- Frequent bathing to remove allergens and control colonization by Staphylococcus and Malassezia
- Immunotherapy (hyposensitization)
- Allergens selected based on the results of intradermal testing or allergen-specific IgE serology
- Injectable or sublingual immunotherapy(SLIT)
- About 2/3 dogs show some response to therapy
- May take up to a year of therapy before improvement is seen
COMMENTS
- Best practices for control of AD are early diagnosis and establishment of a management program
- Controlling flare factors such as skin infections and fleas is essential
- Client education about the pathogenesis and ongoing nature of AD is key to successful management.
- Consider referral to a local dermatologist
References:
- Miller WH, Griffin CE. Campbell K. eds. Muller and Kirk’s Small Animal Dermatology 7th ed. Saunders, 2013: 125. 364-388
- Veterinary Clinical Advisor. Dogs and Cats. Cote.E. 2nd ed. Mosby. 2011: 106-108
- Nuttall T, Harvey RG, McKeever PJ. A Colour Handbook of Skin Disease Of The Dog and Cat. 2nd ed. 2009 Manson Publishing, 20-30.
abscess
A discrete swelling containing purulent material, typically in the subcutis

Perianal abscess in a dog
alopecia
Absence of hair from areas where it is normally present; may be due to folliculitis, abnormal follicle cycling, or self-trauma

Extensive alopecia secondary to cutaneous epitheliotropic lymphoma
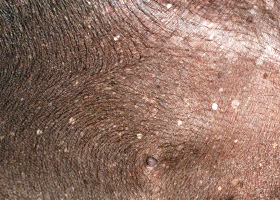
alopecia (“moth-eaten”)
well-circumscribed, circular, patchy to coalescing alopecia, often associated with folliculitis

“Moth-eaten” alopecia secondary to superficial bacterial folliculitis




hemorrhagic bullae
Blood-filled elevation of epidermis, >1cm

Interdigital hemorrhagic bulla in a dog with deep pyoderma and furunculosis
comedo
dilated hair follicle filled with keratin, sebum
Comedones on the ventral abdomen of a dog with hypercortisolism
crust
Dried exudate and keratinous debris on skin surface

Multifocal crusts due to pemphigus foliaceus



epidermal collarettes
Circular scale or crust with erythema, associated with folliculitis or ruptured pustules or vesicles

Epidermal collarettes in a dog with Staphylococcus superficial bacterial folliculitis
erosion
Defect in epidermis that does not penetrate basement membrane. Histopathology may be needed to differentiate from ulcer.

Erosions in a dog with vasculitis
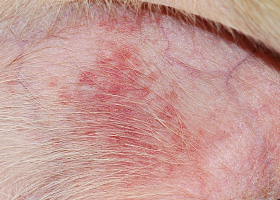
erythema
Red appearance of skin due to inflammation, capillary congestion

Erythema in a dog with cutaneous drug eruption
eschar
Thick crust often related to necrosis, trauma, or thermal/chemical burn

Eschar from physical trauma
excoriation
Erosions and/or ulcerations due to self-trauma

Excoriations in a cat with atopic dermatitis
fissure
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Fissures of the footpads in a dog with superficial necrolytic dermatitis
fistula
Ulcer on skin surface that originates from and is contiguous with tracts extending into deeper, typically subcutaneous tissues

Perianal fistulas in a dog
follicular casts
Accumulation of scale adherent to hair shaft

Follicular casts surrounding hairs from a dog with hypothyroidism
hyperkeratosis
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Idiopathic hyperkeratosis of the nasal planum (left) and footpads (right)
hyperpigmentation
Increased melanin in skin, often secondary to inflammation

Inflammatory lesions (left) resulting in post-inflammatory hyperpigmentation (right)

hypotrichosis
Lack of hair due to genetic factors or defects in embryogenesis.

Congenital hypotrichosis in chocolate Labrador puppies.

lichenification
Thickening of the epidermis, often due to chronic inflammation resulting in exaggerated texture

Lichenification of skin in a dog with chronic atopic dermatitis and Malassezia dermatitis
macule
Flat lesion associated with color change <1cm

Pigmented macule (left) Erythematous macule (right)
melanosis
Increased melanin in skin, may be secondary to inflammation.

Post inflammatory hyperpigmentation of this dog’s thigh
miliary
Multifocal, papular, crusting dermatitis; a descriptive term, not a diagnosis

Miliary dermatitis in a flea allergic cat
morbiliform
A erythematous, macular, papular rash; the erythematous macules are typically 2-10 mm in diameter with coalescence to form larger lesions in some areas

Morbiliform eruptions in a dog with a cutaneous drug reaction

onychodystrophy
Abnormal nail morphology due to nail bed infection, inflammation, or trauma; may include: Onychogryphosis, Onychomadesis, Onychorrhexis, Onychoschizia

Onychodystrophy in dog with chronic allergies
onychogryphosis
Abnormal claw curvature; secondary to nail bed inflammation or trauma

Onychogryphosis in a dog with symmetric lupoid onychodystrophy
onychomadesis
Claw sloughing due to nail bed inflammation or trauma

Onychomadesis in a dog with symmetric lupoid onychodystrophy
onychorrhexis
Claw fragmentation due to nail bed inflammation or trauma

Onychorrhexis in a dog with symmetric lupoid onychodystrophy
onychoschizia
Claw splitting due to nail bed inflammation or trauma

Onychoschizia in a dog with symmetric lupoid onychodystrophy

patch
Flat lesion associated with color change >1cm

Hypopigmented patch (left), erythematous patch (right)
petechiae
Small erythematous or violaceous lesions due to dermal bleeding

Petechiae in a dog with cutaneous vasculitis
phlebectasia
Venous dilation; most commonly associated with hypercortisolism

Phlebectasia and cutaneous atrophy due to hypercortisolism in a dog
plaques
Flat-topped elevation >1cm formed of coalescing papules or dermal infiltration

Plaques in a cat with cutaneous lymphoma
pustule
Raised epidermal infiltration of pus

Pustules on the abdomen of a dog with superficial staphylococcal pyoderma.
scale
Accumulation of loose fragments of stratum corneum

Loose, large scales due to ichthyosis in a Golden Retriever
scar
Fibrous tissue replacing damaged cutaneous and/or subcutaneous tissues

Scarring (right) following the healing of an ulcer (left) in a dog with sterile nodular dermatitis
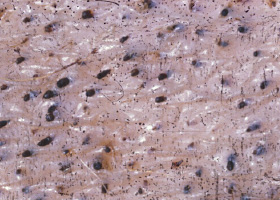
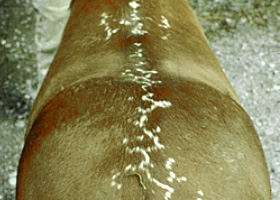
serpiginous
Undulating, serpentine (snake-like) arrangement of lesions

Serpiginous urticarial lesions on a horse
telangiectasia
Permanent enlargement of vessels resulting in a red or violet lesion (rare)

Telangiectasia in a dog with angiomatosis
ulcer
A defect in epidermis that penetrates the basement membrane. Histopathology may be needed to differentiate from an erosion.

Ulcerations of the skin of a dog with vasculitis.
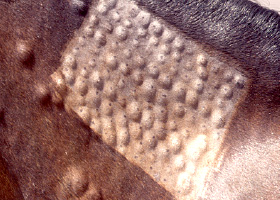
urticaria
Wheals (steep-walled, circumscribed elevation in the skin due to edema ) due to hypersensitivity reaction

Urticaria in a horse
vesicle
Fluid-filled elevation of epidermis, <1cm

Vesicles and bullae on ear pinna due to bullous pemphigoid
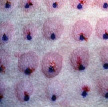
wheal
Steep-walled, circumscribed elevation in the skin due to edema
Wheals associated with intradermal allergy testing in a horse