ALLERGIC DERMATOSES : FLEA ALLERGY DERMATITIS (FAD)
- At a glance
- WHAT DOES IT LOOK LIKE?
- WHAT ELSE LOOKS LIKE THIS?
- HOW DO I DIAGNOSE IT?
- HOW DO I MANAGE IT?
- COMMENTS
At A Glance
- The most common pruritic skin disease of dogs and cats
- Flea saliva contains amino acids, aromatic compounds, fluorescent materials, polypeptides, and phosphorus
- When fleas feed, proteins in flea saliva are released into the skin of the pet
- Numerous immunologic responses, including immediate and delayed hypersensitivity to the flea saliva, are responsible for the clinical signs; therefore just having fleas present does not mean hypersensitivity exists
- Dogs with atopic dermatitis seem to be predisposed to FAD; otherwise no breed, sex, or age predilection exists










WHAT DOES IT LOOK LIKE?
- Tail-head pruritus extending to the lumbo-sacral area, ventral abdomen, caudal and medial thighs with erythema, evidence of self-trauma, hyperpigmentation, lichenification
- Papule and crust may be evident
- Common manifestations in cats include miliary dermatitis, indolent ulcer, eosinophilic plaques, linear granulomas and symmetrical alopecia
- Disease can be seasonal or non-seasonal, depending on the pet's geographic location and housing
- Secondary superficial and sometimes deep pyoderma can result from self-trauma
What Else Looks Like This?
- Food allergy
- Atopic dermatitis
- Cheyletiella infestation
- Bacterial folliculitis and pyoderma
- Malassezia dermatitis
- Sarcoptic mange
- Pediculosis (lice)
- Endocrinopathies (hyperadrenocorticism, hypothyroidism)
How Do I Diagnose It?
- Demonstration of fleas (sometimes difficult in pets that ingest the fleas) and flea dirt (feces/digested blood)
- Resolution of clinical signs with successful flea control program
- Intradermal test with flea extract can show immediate (within 20 minutes) or delayed (48 hrs) reaction of a wheal – positive reactions can occur in clinically normal dogs, however false positives are possible, and delayed reactions may be subtle and hard to recognize (biopsy may be required)


How Do I Manage It?
- Flea control – the most important consideration is to treat ALL pets in the home (indoor and outdoor animals) AND the environment, both indoors and out
- Treating secondary infections
- JAK Inhibitor: A different class of medication that specifically targets the cytokines involved in itch and inflammation associated with allergic skin conditons with minimal negative impact on immune function
- Controlling pruritus with a short course of oral glucocorticoids
| INSERT FLEA PRODUCT CHART | ||||
|---|---|---|---|---|
| CHEMICAL | MECHANISM OF ACTION | TYPE | AVAILABLE | USE |
| flumethrin |
a pyrethroid that is combined with imidacloprid in a slow-release polymer
|
A
|
C
|
P
|
| imidacloprid |
nicotinic Ach- receptor antagonist
|
A
|
T
|
P
|
| lufenuron |
inhibits chitin synthesis
|
GR
|
O , I
|
P
|
| (S)-methoprene |
juvenile hormone analog
|
GR
|
T, C
|
E, P
|
| nitenpyram |
nicotinic Ach receptor antagonist
|
A
|
O
|
P
|
| permethrin |
pyrethroid – sodium channel modulator
|
A
|
T
|
P (NOT FOR CATS); E
|
| pyrethrin |
pyrethroid-sodium channel modulator
|
A
|
T
|
P
|
| pyriproxyfen |
juvenile hormone analog
|
GR
|
T
|
P
|
| selamectin |
avermectin derivative – chloride channel activator
|
A /L/O
|
T/S
|
P
|
| spinosad |
nicotinic Ach receptor agonist
|
A
|
O
|
P
|
| fluralaner |
Ligand gated chloride channels
|
A
|
O
|
P
|
| afoxalaner |
GABA (gamma aminobutyric acid)–modulated chloride channels
|
A
|
O
|
P
|
Environmental Control
- Adulticide/Larvacide/Ovicidal
- Vacuuming, including the vehicle if the pet is transported
- Washing pet’s bedding or other areas where the pet sleeps
- Removing organic debris (old leaves) and limiting pet access to areas that promote flea growth (temperature 23ºC/73ºF and relative humidity of 78%)
- Steinerema carpocapsae – nematodes that kill flea larvae in grass and soil
Comments
- Many dogs and cats that are flea allergic have very few fleas on them—dogs and cats ingest fleas and also remove them by incessant scratching
- The most common flea infesting dogs and cats is Ctenocephalides felis felis
- Fleas are highly prolific—females begin egg production 24 hours after consuming a blood meal and may produce 20-50 eggs per day for over 100 days; a single mated pair can produce over 20,000 adult fleas and 160,000 pre-adult forms in two months
- Flea infested dogs and cats often acquire tapeworms (Diplydium caninum) through ingestion of fleas
- Fleas are also vectors of Rickettsia felis, Rickettsia typhi, Bartonella hensalae, Bartonella clarridgeiae and other organisms
- Female fleas consume blood at a rate of 10-15 times their body weight each day
- Warn clients that permethrin-containing products may kill cats and fipronil is toxic to rabbits
- Bevier, D. Flea Allergy Dermatitis in Small Animal Dermatology Secrets, KL Campbell, 2004, pp 208- 213.
- Hnilica KA. Small Animal Dermatology. A color atlas and therapeutic Guide, 3rd ed. 2011; pp 183-188.
- Miller, WH et al. Muller and Kirk’s Small Animal Dermatology, 7th ed. pp 405-410.
- Morgan RV ed, Handbook of Small Animal Practice, 5th ed.. 2008 pp 828-829
abscess
A discrete swelling containing purulent material, typically in the subcutis

Perianal abscess in a dog
alopecia
Absence of hair from areas where it is normally present; may be due to folliculitis, abnormal follicle cycling, or self-trauma

Extensive alopecia secondary to cutaneous epitheliotropic lymphoma
alopecia (“moth-eaten”)
well-circumscribed, circular, patchy to coalescing alopecia, often associated with folliculitis

“Moth-eaten” alopecia secondary to superficial bacterial folliculitis




hemorrhagic bullae
Blood-filled elevation of epidermis, >1cm

Interdigital hemorrhagic bulla in a dog with deep pyoderma and furunculosis
comedo
dilated hair follicle filled with keratin, sebum
Comedones on the ventral abdomen of a dog with hypercortisolism
crust
Dried exudate and keratinous debris on skin surface

Multifocal crusts due to pemphigus foliaceus



epidermal collarettes
Circular scale or crust with erythema, associated with folliculitis or ruptured pustules or vesicles

Epidermal collarettes in a dog with Staphylococcus superficial bacterial folliculitis
erosion
Defect in epidermis that does not penetrate basement membrane. Histopathology may be needed to differentiate from ulcer.

Erosions in a dog with vasculitis
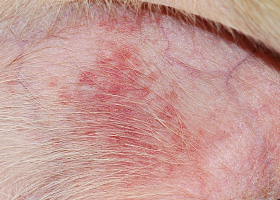
erythema
Red appearance of skin due to inflammation, capillary congestion

Erythema in a dog with cutaneous drug eruption
eschar
Thick crust often related to necrosis, trauma, or thermal/chemical burn

Eschar from physical trauma
excoriation
Erosions and/or ulcerations due to self-trauma

Excoriations in a cat with atopic dermatitis
fissure
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Fissures of the footpads in a dog with superficial necrolytic dermatitis
fistula
Ulcer on skin surface that originates from and is contiguous with tracts extending into deeper, typically subcutaneous tissues

Perianal fistulas in a dog
follicular casts
Accumulation of scale adherent to hair shaft

Follicular casts surrounding hairs from a dog with hypothyroidism
hyperkeratosis
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Idiopathic hyperkeratosis of the nasal planum (left) and footpads (right)
hyperpigmentation
Increased melanin in skin, often secondary to inflammation

Inflammatory lesions (left) resulting in post-inflammatory hyperpigmentation (right)

hypotrichosis
Lack of hair due to genetic factors or defects in embryogenesis.

Congenital hypotrichosis in chocolate Labrador puppies.

lichenification
Thickening of the epidermis, often due to chronic inflammation resulting in exaggerated texture

Lichenification of skin in a dog with chronic atopic dermatitis and Malassezia dermatitis
macule
Flat lesion associated with color change <1cm

Pigmented macule (left) Erythematous macule (right)
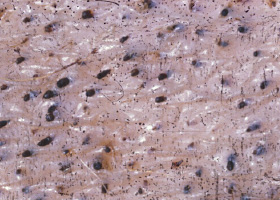
melanosis
Increased melanin in skin, may be secondary to inflammation.

Post inflammatory hyperpigmentation of this dog’s thigh
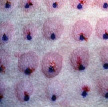
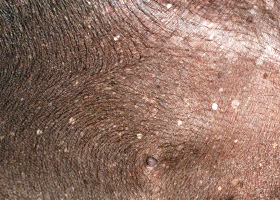
miliary
Multifocal, papular, crusting dermatitis; a descriptive term, not a diagnosis

Miliary dermatitis in a flea allergic cat
morbiliform
A erythematous, macular, papular rash; the erythematous macules are typically 2-10 mm in diameter with coalescence to form larger lesions in some areas

Morbiliform eruptions in a dog with a cutaneous drug reaction

onychodystrophy
Abnormal nail morphology due to nail bed infection, inflammation, or trauma; may include: Onychogryphosis, Onychomadesis, Onychorrhexis, Onychoschizia

Onychodystrophy in dog with chronic allergies
onychogryphosis
Abnormal claw curvature; secondary to nail bed inflammation or trauma

Onychogryphosis in a dog with symmetric lupoid onychodystrophy
onychomadesis
Claw sloughing due to nail bed inflammation or trauma

Onychomadesis in a dog with symmetric lupoid onychodystrophy
onychorrhexis
Claw fragmentation due to nail bed inflammation or trauma

Onychorrhexis in a dog with symmetric lupoid onychodystrophy
onychoschizia
Claw splitting due to nail bed inflammation or trauma

Onychoschizia in a dog with symmetric lupoid onychodystrophy

patch
Flat lesion associated with color change >1cm

Hypopigmented patch (left), erythematous patch (right)
petechiae
Small erythematous or violaceous lesions due to dermal bleeding

Petechiae in a dog with cutaneous vasculitis
phlebectasia
Venous dilation; most commonly associated with hypercortisolism

Phlebectasia and cutaneous atrophy due to hypercortisolism in a dog
plaques
Flat-topped elevation >1cm formed of coalescing papules or dermal infiltration

Plaques in a cat with cutaneous lymphoma
pustule
Raised epidermal infiltration of pus

Pustules on the abdomen of a dog with superficial staphylococcal pyoderma.
scale
Accumulation of loose fragments of stratum corneum

Loose, large scales due to ichthyosis in a Golden Retriever
scar
Fibrous tissue replacing damaged cutaneous and/or subcutaneous tissues

Scarring (right) following the healing of an ulcer (left) in a dog with sterile nodular dermatitis
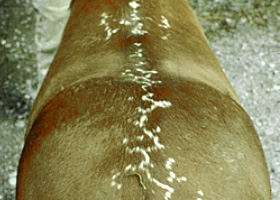
serpiginous
Undulating, serpentine (snake-like) arrangement of lesions

Serpiginous urticarial lesions on a horse
telangiectasia
Permanent enlargement of vessels resulting in a red or violet lesion (rare)

Telangiectasia in a dog with angiomatosis
ulcer
A defect in epidermis that penetrates the basement membrane. Histopathology may be needed to differentiate from an erosion.

Ulcerations of the skin of a dog with vasculitis.
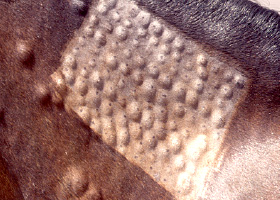
urticaria
Wheals (steep-walled, circumscribed elevation in the skin due to edema ) due to hypersensitivity reaction

Urticaria in a horse
vesicle
Fluid-filled elevation of epidermis, <1cm

Vesicles and bullae on ear pinna due to bullous pemphigoid
wheal
Steep-walled, circumscribed elevation in the skin due to edema
Wheals associated with intradermal allergy testing in a horse