ALLERGIC DERMATOSES : FOOD ALLERGY (CARF) - CANINE
- At a glance
- WHAT DOES IT LOOK LIKE?
- WHAT ELSE LOOKS LIKE THIS?
- HOW DO I DIAGNOSE IT?
- HOW DO I MANAGE IT?
- COMMENTS
Animal Allergy and Dermatology Service of Connecticut
At A Glance:
- Non-seasonal pruritic allergic skin disease associated with ingestion of offending allergen in pet’s diet (the most frequently fed ingredients)
- Usually non-life threatening, unlike in humans who may die if consume a food allergen
- Exact pathogenesis in the dog is not completely understood; may include a variety of immunological reactions (Type I, Type III, and/or Type IV)
- An abnormal immunologic reaction, most often to food glycoprotein- usually heat stable, water soluble 10-70 kDal in size
- Often diagnosed in conjunction with atopic dermatitis (AD) in the dog (not exclusive of AD)
- The third most common allergic disease in the dog (10-15%) after flea allergy dermatitis and atopic dermatitis



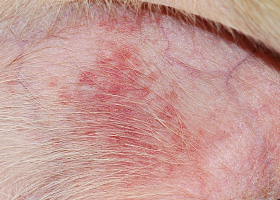
Excoriations on the ear and face of a food allergic dog with moist secondary pyoderma.




What Does It Look Like?
- No age or sex predilection, but many cases begin at less than 1 year of age, and more common than AD in dogs younger than 6 months
- Any breed can be affected but reported predisposed breeds include: American cocker spaniel, English springer spaniel, Labrador retriever, collie, miniature schnauzer, Chinese shar pei, poodle, West Highland white terrier, boxer, dachshund, Dalmatian, Lhasa apso, German shepherd dog, Rhodesian ridgeback, pug, and golden retriever
- Distribution of clinical signs are similar to AD – face, ears, axillae, inguinal area, abdomen; pattern with pruritus of mainly ears and perineal area (“ears and rears”) is often attributed to CARF (24%)
- Concurrent gastrointestinal signs – 10-30%; flatulence and increased frequency of defecation occur more commonly than vomiting or diarrhea
- Recurrent secondary staphylococcal (pruritic or non-pruritic) dermatitis and yeast (Malassezia) infections can occur
- Rarely, vasculitis, urticaria and erythema multiforme
What Else Looks Like This?
- Atopic dermatitis (non-seasonal)
- Sarcoptic mange
- Staphylococcal / Malassezia infections
- Cheyletiellosis
- Dermatophytosis
- Flea allergy dermatitis
HOW DO I DIAGNOSE IT?
- The only accurate method of diagnosis is a food trial that lasts up to 12 weeks during which time the pet’s clinical signs resolve (followed by recurrence of signs upon provocation—see below)
- This diet can be home-cooked or carefully selected prescription prepared food
- There is insufficient evidence that blood or skin testing for food allergies is diagnostic
- Ingredients must be novel proteins for the pet or hydrolyzed proteins (proteins broken down to peptides smaller than 10kDa)
- All treats, chewable medications (including parasite preventatives and NSAIDs) must be replaced with non-flavored versions or topical therapy where appropriate
- If pruritus resolves with the trial, a food challenge (provocation for up to two weeks) should be done to confirm the offending protein. This can be done with the initial diet, with ingredients from that diet, or specific treats. Once the offending protein is identified, avoiding its ingestion is the goal of long-term management.


How Do I Manage It?
- Once it is determined that the dermatitis is due to a reaction to something the pet has been fed, avoiding its ingestion is the goal of long-term management
- JAK Inhibitor: A different class of medication that specifically targets the cytokines involved in itch and inflammation associated with allergic skin conditons with minimal negative impact on immune function
- Pruritus associated with CARFs generally has partial to no response to treatment with corticosteroids and/or cyclosporine (some animals show a partial response and then relapse when dose is tapered)
Comments:
- Cross-reactions may occur among foods within a food group (e.g., beef and venison) and also between food allergens and other allergens (e.g., milk and beef; crustaceans and cockroaches; birch pollen may cross-react with a variety of fruits and vegetables) Beef has been reported as the most common reactant in dogs, followed by soy, chicken, milk, corn, wheat and eggs
- Hydrolyzed diets may work best for dogs with immediate (Type I) hypersensitivity reactions and may not work for dogs with delayed CAFR
- More than one elimination diet trial may be required to diagnose a CAFR
- If a home-cooked diet is used long-term consultation with a nutritionist is necessary to ensure the diet is nutritionally adequate for the patient
References:
- Bruner, S. Dietary Hypersensitivty, in Small Animal Dermatology Secrets, KL Campbell, 2004, pp 196-201.
- Handbook of Small Animal Practice, 5th ed. Morgan, RV, ed. 2008 pp 825-826.
- Miller, WH et al. Muller and Kirk’s Small Animal Dermatology, 7th ed. pp 397-404.
abscess
A discrete swelling containing purulent material, typically in the subcutis

Perianal abscess in a dog
alopecia
Absence of hair from areas where it is normally present; may be due to folliculitis, abnormal follicle cycling, or self-trauma

Extensive alopecia secondary to cutaneous epitheliotropic lymphoma
alopecia (“moth-eaten”)
well-circumscribed, circular, patchy to coalescing alopecia, often associated with folliculitis

“Moth-eaten” alopecia secondary to superficial bacterial folliculitis




hemorrhagic bullae
Blood-filled elevation of epidermis, >1cm

Interdigital hemorrhagic bulla in a dog with deep pyoderma and furunculosis
comedo
dilated hair follicle filled with keratin, sebum
Comedones on the ventral abdomen of a dog with hypercortisolism
crust
Dried exudate and keratinous debris on skin surface

Multifocal crusts due to pemphigus foliaceus



epidermal collarettes
Circular scale or crust with erythema, associated with folliculitis or ruptured pustules or vesicles

Epidermal collarettes in a dog with Staphylococcus superficial bacterial folliculitis
erosion
Defect in epidermis that does not penetrate basement membrane. Histopathology may be needed to differentiate from ulcer.

Erosions in a dog with vasculitis
erythema
Red appearance of skin due to inflammation, capillary congestion

Erythema in a dog with cutaneous drug eruption
eschar
Thick crust often related to necrosis, trauma, or thermal/chemical burn

Eschar from physical trauma
excoriation
Erosions and/or ulcerations due to self-trauma

Excoriations in a cat with atopic dermatitis
fissure
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Fissures of the footpads in a dog with superficial necrolytic dermatitis
fistula
Ulcer on skin surface that originates from and is contiguous with tracts extending into deeper, typically subcutaneous tissues

Perianal fistulas in a dog
follicular casts
Accumulation of scale adherent to hair shaft

Follicular casts surrounding hairs from a dog with hypothyroidism
hyperkeratosis
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Idiopathic hyperkeratosis of the nasal planum (left) and footpads (right)
hyperpigmentation
Increased melanin in skin, often secondary to inflammation

Inflammatory lesions (left) resulting in post-inflammatory hyperpigmentation (right)

hypotrichosis
Lack of hair due to genetic factors or defects in embryogenesis.

Congenital hypotrichosis in chocolate Labrador puppies.

lichenification
Thickening of the epidermis, often due to chronic inflammation resulting in exaggerated texture

Lichenification of skin in a dog with chronic atopic dermatitis and Malassezia dermatitis
macule
Flat lesion associated with color change <1cm

Pigmented macule (left) Erythematous macule (right)
melanosis
Increased melanin in skin, may be secondary to inflammation.

Post inflammatory hyperpigmentation of this dog’s thigh
miliary
Multifocal, papular, crusting dermatitis; a descriptive term, not a diagnosis

Miliary dermatitis in a flea allergic cat
morbiliform
A erythematous, macular, papular rash; the erythematous macules are typically 2-10 mm in diameter with coalescence to form larger lesions in some areas

Morbiliform eruptions in a dog with a cutaneous drug reaction

onychodystrophy
Abnormal nail morphology due to nail bed infection, inflammation, or trauma; may include: Onychogryphosis, Onychomadesis, Onychorrhexis, Onychoschizia

Onychodystrophy in dog with chronic allergies
onychogryphosis
Abnormal claw curvature; secondary to nail bed inflammation or trauma

Onychogryphosis in a dog with symmetric lupoid onychodystrophy
onychomadesis
Claw sloughing due to nail bed inflammation or trauma

Onychomadesis in a dog with symmetric lupoid onychodystrophy
onychorrhexis
Claw fragmentation due to nail bed inflammation or trauma

Onychorrhexis in a dog with symmetric lupoid onychodystrophy
onychoschizia
Claw splitting due to nail bed inflammation or trauma

Onychoschizia in a dog with symmetric lupoid onychodystrophy

patch
Flat lesion associated with color change >1cm

Hypopigmented patch (left), erythematous patch (right)
petechiae
Small erythematous or violaceous lesions due to dermal bleeding

Petechiae in a dog with cutaneous vasculitis
phlebectasia
Venous dilation; most commonly associated with hypercortisolism

Phlebectasia and cutaneous atrophy due to hypercortisolism in a dog
plaques
Flat-topped elevation >1cm formed of coalescing papules or dermal infiltration

Plaques in a cat with cutaneous lymphoma
pustule
Raised epidermal infiltration of pus

Pustules on the abdomen of a dog with superficial staphylococcal pyoderma.
scale
Accumulation of loose fragments of stratum corneum

Loose, large scales due to ichthyosis in a Golden Retriever
scar
Fibrous tissue replacing damaged cutaneous and/or subcutaneous tissues

Scarring (right) following the healing of an ulcer (left) in a dog with sterile nodular dermatitis
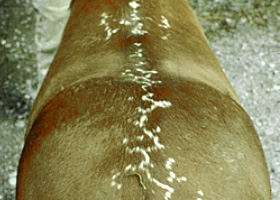
serpiginous
Undulating, serpentine (snake-like) arrangement of lesions

Serpiginous urticarial lesions on a horse
telangiectasia
Permanent enlargement of vessels resulting in a red or violet lesion (rare)

Telangiectasia in a dog with angiomatosis
ulcer
A defect in epidermis that penetrates the basement membrane. Histopathology may be needed to differentiate from an erosion.

Ulcerations of the skin of a dog with vasculitis.
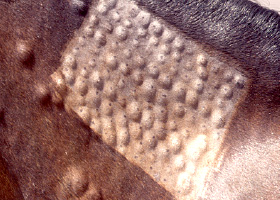
urticaria
Wheals (steep-walled, circumscribed elevation in the skin due to edema ) due to hypersensitivity reaction

Urticaria in a horse
vesicle
Fluid-filled elevation of epidermis, <1cm

Vesicles and bullae on ear pinna due to bullous pemphigoid
wheal
Steep-walled, circumscribed elevation in the skin due to edema
Wheals associated with intradermal allergy testing in a horse