LUPOID ONYCHODYSTROPHY
- At a glance
- WHAT DOES IT LOOK LIKE?
- WHAT ELSE LOOKS LIKE THIS?
- HOW DO I DIAGNOSE IT?
- HOW DO I MANAGE IT?
- COMMENTS
AT A GLANCE
- The most common inflammatory disease to cause abnormal claws
- The cause of this condition is unknown but is suspected to be hereditary, inflammatory or immune-mediated
- Normally involves multiple nails/claws on all four feet
- Uncommon to rare in dogs
- Most commonly seen in middle aged dogs, 3-8 years of age
- Predisposed breeds include the German Shepherd dog, Rottweiler and Gordon Setter






WHAT DOES IT LOOK LIKE?
- Often starts as an acute onset of claw loss
- May be associated with significant inflammation or purulent discharge from nailbeds
- May also present as dry, distorted claws that do not slough on their own
- Typically, one or two claws are lost first, followed by sloughing of all claws within several weeks to months
- One or more of the following abnormalities are seen over time
- Onychogryphosis- abnormal curvature of the claws
- Onychomadesis- sloughing of claws
- Onychorrhexis- fragmentation of the claws
- Onychoschizia- splitting of the claws
- Inflammation of the nail fold (paronychia) is uncommon unless there is a secondary bacterial infection present
- Other skin abnormalities and systemic illness are not seen
- Dogs with this disease may be asymptomatic or have associated lameness
WHAT ELSE LOOKS LIKE THIS?
- Bacterial claw infection
- Dermatophytosis/deep fungal infection
- Immune-mediated diseases:
- Pemphigus vulgaris
- Bullous pemphigoid
- Lupus erythematosus
- Vasculitis
- Drug eruption
- Neoplasia (squamous cell carcinoma)
- Cryoglobulinemia or cold agglutinin disease
HOW DO I DIAGNOSE IT?
- History and clinical signs
- Fungal culture to rule out dermatophytosis
- Skin cytology/culture if significant paronychia is noted
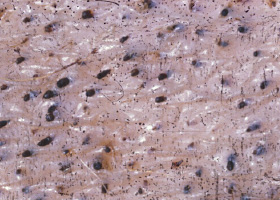
- Surgical amputation or biopsy of an affected P3 for dermatohistopathology:
- Hydropic degeneration of the basal cell layer
- Lichenoid interface dermatitis
- Pigmentary incontinence
HOW DO I MANAGE IT?
General information
- Treatment will often take up to 12 weeks to see significant clinical response
- If there is minimal response after 6-8 weeks, medications can added to the current protocol or changed altogether
- Treatment should be continued for a minimum of 6 months but may be necessary for the rest of the dog’s life
Specific treatments
- Manual removal of loose claws (general anesthesia recommended)
- Omega-3 and omega-6 fatty acids
- 180mg EPA/5 kg every 24 hours
- Often used in combination with vitamin E
- Vitamin E
- 200-400 IU by mouth every 12 hours
- Tetracycline/Niacinamide
- Dogs weighing less than 10kg- 250mg of each by mouth every 8 hours
- Dogs weighing more than 10kg- 500mg of each by mouth every 8 hours
- This can be tapered to every 12 hours after noticeable nail regrowth
- Doxycycline at 5-10 mg/kg by mouth every12-24h can be used in place of tetracycline
- Pentoxifylline
- 10-25mg/kg by mouth every 8-12 hours
- Cyclosporine
- 5-10 mg/kg by mouth every 24 hours
- Tapered to lowest dose possible that prevents relapse
- Prednisone
- Often reserved for cases that have failed other treatments
- 2-4 mg/kg/day for approximately 2-4 weeks, then tapered slowly to reach the lowest every other dose that prevents relapse
- Azathioprine
- 1.1-2.2 mg/kg by mouth every 24 to 48 hours
- Monitor CBC and liver enzymes every 2 weeks until disease is in remission and dose has been decreased
- Frequent trimming of claws (about every 2 weeks) to prevent further cracks
- Treatment with appropriate antibiotics if secondary bacterial paronychia is present
- Onychectomy may be considered for refractory cases associated with onychalgia (pain)
- Consider a food elimination trial if there is an suspicion of an adverse food reaction based on history and diagnostics
- Overall prognosis is good but claws may continue to break easily and remain deformed
COMMENTS
- Also called symmetric lupoid onychitis due to the presence of inflammation involving the claws
- Lupoid onychodystrophy is the most common inflammatory disease that leads to abnormal claws and eventual claw loss.
- Diagnosis is often based on history and clinical signs although surgical removal and histopathology of an affected P3 is helpful for definitive diagnosis
- A variety of therapies can be used- one or multiple modalities of treatments can be used to treat the condition
- It will often take up to 3 months of treatment to see significant clinical response
- Some dogs will need lifelong therapy to maintain remission
Further Reading and References
- Hnilica KA. Symmetrical Lupoid Onychodystrophy. In: Small Animal Dermatology- A Color Atlas and Therapeutic Guide. 3rd Edition. St. Louis: WB Saunders, 2011. p 425-427..
- Miller WH Jr, Griffin CE, Campbell KL. Symmetric Lupoid Onychitis. In: Muller and Kirk’s Small Animal Dermatology. 7th edition. Philadelphia: WB Saunders; 2013. p. 734-739.
abscess
A discrete swelling containing purulent material, typically in the subcutis

Perianal abscess in a dog
alopecia
Absence of hair from areas where it is normally present; may be due to folliculitis, abnormal follicle cycling, or self-trauma

Extensive alopecia secondary to cutaneous epitheliotropic lymphoma
alopecia (“moth-eaten”)
well-circumscribed, circular, patchy to coalescing alopecia, often associated with folliculitis

“Moth-eaten” alopecia secondary to superficial bacterial folliculitis




hemorrhagic bullae
Blood-filled elevation of epidermis, >1cm

Interdigital hemorrhagic bulla in a dog with deep pyoderma and furunculosis
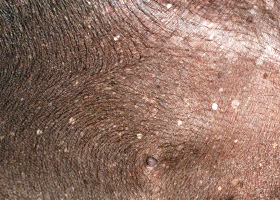
comedo
dilated hair follicle filled with keratin, sebum
Comedones on the ventral abdomen of a dog with hypercortisolism
crust
Dried exudate and keratinous debris on skin surface

Multifocal crusts due to pemphigus foliaceus



epidermal collarettes
Circular scale or crust with erythema, associated with folliculitis or ruptured pustules or vesicles

Epidermal collarettes in a dog with Staphylococcus superficial bacterial folliculitis
erosion
Defect in epidermis that does not penetrate basement membrane. Histopathology may be needed to differentiate from ulcer.

Erosions in a dog with vasculitis
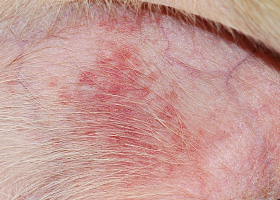
erythema
Red appearance of skin due to inflammation, capillary congestion

Erythema in a dog with cutaneous drug eruption
eschar
Thick crust often related to necrosis, trauma, or thermal/chemical burn

Eschar from physical trauma
excoriation
Erosions and/or ulcerations due to self-trauma

Excoriations in a cat with atopic dermatitis
fissure
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Fissures of the footpads in a dog with superficial necrolytic dermatitis
fistula
Ulcer on skin surface that originates from and is contiguous with tracts extending into deeper, typically subcutaneous tissues

Perianal fistulas in a dog
follicular casts
Accumulation of scale adherent to hair shaft

Follicular casts surrounding hairs from a dog with hypothyroidism
hyperkeratosis
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Idiopathic hyperkeratosis of the nasal planum (left) and footpads (right)
hyperpigmentation
Increased melanin in skin, often secondary to inflammation

Inflammatory lesions (left) resulting in post-inflammatory hyperpigmentation (right)

hypotrichosis
Lack of hair due to genetic factors or defects in embryogenesis.

Congenital hypotrichosis in chocolate Labrador puppies.

lichenification
Thickening of the epidermis, often due to chronic inflammation resulting in exaggerated texture

Lichenification of skin in a dog with chronic atopic dermatitis and Malassezia dermatitis
macule
Flat lesion associated with color change <1cm

Pigmented macule (left) Erythematous macule (right)
melanosis
Increased melanin in skin, may be secondary to inflammation.

Post inflammatory hyperpigmentation of this dog’s thigh
miliary
Multifocal, papular, crusting dermatitis; a descriptive term, not a diagnosis

Miliary dermatitis in a flea allergic cat
morbiliform
A erythematous, macular, papular rash; the erythematous macules are typically 2-10 mm in diameter with coalescence to form larger lesions in some areas

Morbiliform eruptions in a dog with a cutaneous drug reaction

onychodystrophy
Abnormal nail morphology due to nail bed infection, inflammation, or trauma; may include: Onychogryphosis, Onychomadesis, Onychorrhexis, Onychoschizia

Onychodystrophy in dog with chronic allergies
onychogryphosis
Abnormal claw curvature; secondary to nail bed inflammation or trauma

Onychogryphosis in a dog with symmetric lupoid onychodystrophy
onychomadesis
Claw sloughing due to nail bed inflammation or trauma

Onychomadesis in a dog with symmetric lupoid onychodystrophy
onychorrhexis
Claw fragmentation due to nail bed inflammation or trauma

Onychorrhexis in a dog with symmetric lupoid onychodystrophy
onychoschizia
Claw splitting due to nail bed inflammation or trauma

Onychoschizia in a dog with symmetric lupoid onychodystrophy

patch
Flat lesion associated with color change >1cm

Hypopigmented patch (left), erythematous patch (right)
petechiae
Small erythematous or violaceous lesions due to dermal bleeding

Petechiae in a dog with cutaneous vasculitis
phlebectasia
Venous dilation; most commonly associated with hypercortisolism

Phlebectasia and cutaneous atrophy due to hypercortisolism in a dog
plaques
Flat-topped elevation >1cm formed of coalescing papules or dermal infiltration

Plaques in a cat with cutaneous lymphoma
pustule
Raised epidermal infiltration of pus

Pustules on the abdomen of a dog with superficial staphylococcal pyoderma.
scale
Accumulation of loose fragments of stratum corneum

Loose, large scales due to ichthyosis in a Golden Retriever
scar
Fibrous tissue replacing damaged cutaneous and/or subcutaneous tissues

Scarring (right) following the healing of an ulcer (left) in a dog with sterile nodular dermatitis
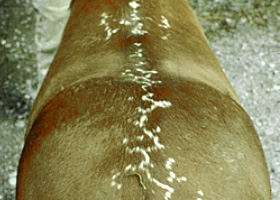
serpiginous
Undulating, serpentine (snake-like) arrangement of lesions

Serpiginous urticarial lesions on a horse
telangiectasia
Permanent enlargement of vessels resulting in a red or violet lesion (rare)

Telangiectasia in a dog with angiomatosis
ulcer
A defect in epidermis that penetrates the basement membrane. Histopathology may be needed to differentiate from an erosion.

Ulcerations of the skin of a dog with vasculitis.
urticaria
Wheals (steep-walled, circumscribed elevation in the skin due to edema ) due to hypersensitivity reaction

Urticaria in a horse
vesicle
Fluid-filled elevation of epidermis, <1cm

Vesicles and bullae on ear pinna due to bullous pemphigoid
wheal
Steep-walled, circumscribed elevation in the skin due to edema
Wheals associated with intradermal allergy testing in a horse