IMMUNE-MEDIATED DERMATOSES : PEMPHIGUS FOLIACEUS
- At a glance
- WHAT DOES IT LOOK LIKE?
- WHAT ELSE LOOKS LIKE THIS?
- HOW DO I DIAGNOSE IT?
- HOW DO I MANAGE IT?
- COMMENTS
AT A GLANCE
- The Pemphigus complex is a group of autoimmune skin diseases
- The most common variant is pemphigus foliaceus (PF)
- Other variants seen in dogs include:
- Pemphigus vulgaris (PV)
- Pemphigus vegetans (PVeg)
- Pemphigus erythematosus (PE)
- Paraneoplastic pemphigus (PNP)
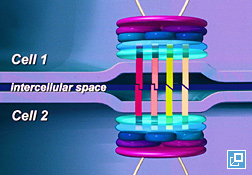
- Autoantibodies are directed against protein antigens in desmosomes which are the intercellular connections between skin cells (keratinocytes) (What Does it Look Like, Figure 1).
For example, in dogs with PF, the autoantodies are thought to be primarily directed at desmocollin 1, whereas in PV they are directed at desmoglein 3. - The precise mechanism by which the autoantibodies breakdown the intercellular connections (a process referred to as acantholysis) is still uncertain.
- Uncommonly, drugs may cause PF in either of 2 syndromes:
- Drug-induced PF: disease goes into remission with drug withdrawal
- Drug-triggered PF: drug initiates disease that persists despite drug withdrawal
- Exposure to sunlight can worsen the lesions of PF
- Breed predilections include Akitas and Chow-chows, although Golden Retrievers, Cocker Spaniels, Dachshunds, Doberman pinschers and English Bulldogs have also been reported to be over-represented.
- The disease typically affects middle age dogs although dogs < 1 year of age have been rarely reported.




WHAT DOES IT LOOK LIKE?
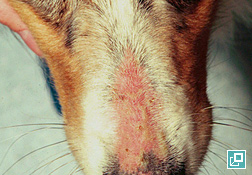
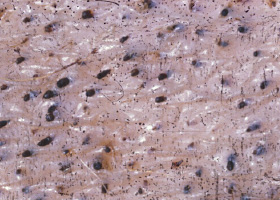
- PF is characteristically a pustular disease (Pathologic Image Library – Figure 2). Pustule are typically large (spanning many hair follicles) but may be smaller (pinpoint) in a minority of cases
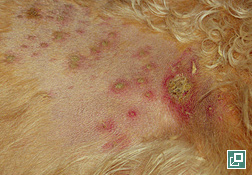
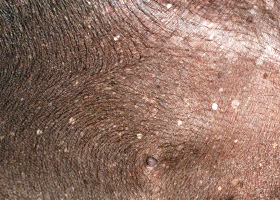
- In some patients, papule (precursor of pustule) are more prominent, while in others there is rapid pustule rupture and the predominant lesions are therefore crust (Pathologic Image Library – Figure 3)
- Post-lesional erosions and alopecia may predominate
- The head, face and ear pinnae are most commonly affected initially with bilateral symmetry
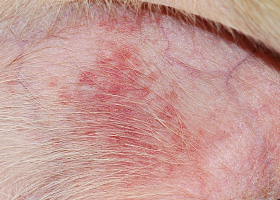
- In most dogs, lesions eventually generalize, sometimes rapidly (Pathologic Image Library – Figure 4)
- The footpads may have significant involvement with crust and fissures, leading to lameness in some patients (Pathologic Image Library – Figure 5)
- The lesions may wax and wane in severity
- Lesions are rarely pruritic
- A few patients are depressed and may have a fever
WHAT ELSE LOOKS LIKE THIS?
- Staphylococcal pyoderma
- Demodicosis
- Dermatophytosis (especially Trichophyton infection)
- Subcorneal pustular dermatosis (very rare)
- Eosinophilic pustulosis (very rare)
- PE (if limited to the head)
- Superficial necrolytic dermatitis
- Zinc-responsive dermatosis
- Cutaneous lymphosarcoma
- Canine distemper
HOW DO I DIAGNOSE IT?
- Superficial pyoderma (negative cytology, negative bacterial culture, lack of response to antibiotic therapy)
- Demodicosis (negative deep skin scraping)
- Dermatophytosis (negative DTM culture)
- Plentiful neutrophils
- Acantholytic cells, especially if present in groups (so called “rafts”)
- Eosinophils may be present or predominate in a few cases
- Absence of coccoid bacteria
- Sample intact and entire pustule for best results. Fresh crust may be useful if pustules are not present
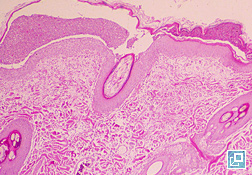
- Subcorneal pustule spanning several hair follicles with neutrophils, acantholytic cells and occasionally eosinophils are characteristic (What Does It Look Like, Pathologic Image Library – Figure 7)
- Neutrophilia may be present but all other values are typically within normal limits.
- Direct immunofluorescence (detection of autoantibodies in the skin) may require submission of fresh frozen skin or in Michels medium; some laboratories perform IHC or DIF on formalin-fixed tissues (contact laboratory)
- Indirect immunofluorescence (detection of circulating autoantibodies) is typically insensitive and inconsistent and is not recommended at this time
HOW DO I MANAGE IT?
- Do no harm!
- Keep patient protected from sunlight
- Consider if the disease may be drug-related and withdraw any suspect drugs
- Frequent bathing (shampoo q 2x weekly) to remove crust
- Topical corticosteroids applied q 12 hrs. Start with more potent corticosteroids (e.g. betamethasone or dexamethasone) until remission is achieved, then convert to less potent corticosteroids for long-term control (e.g. hydrocortisone or prednisolone)
- Topical tacrolimus applied q 12 hrs may also be considered
- Prednisone or prednisolone 1-3 mg/kg q 12-24 hrs (the author typically starts with 1-2 mg/kg q 12 hrs), Significant improvement is typically seen within 2 weeks, then commence slow taper over 2-3 months aiming for a maintenance dose of prednisone < 1 mg/kg q 48 hrs.
- Increase the dose of prednisone/prednisolone if patient is tolerating the drug well
- Change the corticosteroid (triamcinolone or dexamethasone) – beware of increased risk of gastrointestinal side effects. Dexamethasone and triamcinolone are usually dosed at 1/10th the dose of prednisone
- Add azathioprine at 2 mg/kg q 24-48 hrs
- Try the combination of doxycycline ( 5-10 mg/kg q 12 hrs) and niacinamide (dogs < 10 kg 250 mg q 8 hrs; dogs > 10 kg 500 mg q 8 hrs)
- Add cyclosporine (5-10 mg/kg q 24 hrs)
- Human IV immunoglobulin
- Mycophenolate mofetil (10-20 mg/kg q 12 hours)
- Cyclophosphamide (2.2 mg/kg q 48 hrs)
- Chlorambucil (0.1-0.2 mg/kg q 24-48 hrs)
COMMENTS
- PF is the most common autoimmune skin disease of dogs
- Typically middle-aged dogs are affected with Akitas and Chow-chows being particularly predisposed
- PF is a pustular to crusting dermatitis affecting the head and pinnae initially but then generalizes
- Diagnosis is determined by cytology and histopathology
- The prognosis for the disease is good although treatments may have significant side effects and are long term
- August JR, Chickering WR. Pemphigus foliaceus causing lameness in four dogs. Compend Contin Educ Pract Vet 1985; 7: 894-902.
- Gomez SM, Morris DO, Rosenbaum MR, et al. Outcome and complications associated with treatment of pemphigus foliaceus in dogs: 43 cases (1994-2000). J Am Vet Med Assoc 2004; 224(8): 1312-1316.
- Gross TL, Ihrke PE, Walder EJ, et al. Pustular diseases of the epidermis. Skin diseases of the dog and cat. 2nd ed. Ames, Iowa: Blackwell, 2005; 3-26.
- Ihrke PJ, Stannard AA, Ardans AA, et al. Pemphigus foliaceus in dogs: a review of 37 cases. J Am Vet Med Assoc 1985; 186(1): 59-66.
- Ihrke PJ, Stannard AA, Ardans AA, et al. Pemphigus foliaceus of the footpads in three dogs. J Am Vet Med Assoc 1985; 186(1): 67-69.
- Miller WH, Griffin CE, Campbell KL. Autoimmune and immune-mediated dermatoses. Muller and Kirk’s Small animal dermatology (7th ed). St. Louis MO.: Elsevier Mosby, 2013; 432-500.
- Mueller RS, Krebs I, Power HT, et al. Pemphigus foliaceus in 91 dogs. J Am Anim Hosp Assoc 2006; 42 (3):189-196.
- Olivry T. A review of autoimmune skin diseases in animals: I—superficial pemphigus. Vet Dermatol 2006; 17(5):291-305.
- Olivry T, Dunston SM, Walker RH, et al. Investigations on the nature and pathogenicity of circulating antikeratinocyte antibodies in dogs with pemphigus foliaceus. Vet Dermatol 2008; 20(1):42-50.
- Peters J, Scott DW, Erb HN, et al. Comparative analysis of canine dermatophytosis and superficial pemphigus for the prevalence of dermatophytes and acantholytic keratinocytes: a histopathological and clinical retrospective study. Vet Dermatol 2007; 18(4):234-240.
- Rosenkrantz WS. Pemphigus: current therapy. Vet Dermatol 2004; 15(2):90-98.
- Tater KC, Olivry T. Canine and feline Pemphigus foliaceus: Improving your chances of a successful outcome. Vet Med 2010; January: 18-30.
- Yabuzoe A, Shimizu A, Nishifuji K, et al. Canine pemphigus foliaceus antigen is localized within desmosomes of keratinocyte. Vet Immunol Immunopathol 2009; 127(1-2):57-64.
abscess
A discrete swelling containing purulent material, typically in the subcutis

Perianal abscess in a dog
alopecia
Absence of hair from areas where it is normally present; may be due to folliculitis, abnormal follicle cycling, or self-trauma

Extensive alopecia secondary to cutaneous epitheliotropic lymphoma
alopecia (“moth-eaten”)
well-circumscribed, circular, patchy to coalescing alopecia, often associated with folliculitis

“Moth-eaten” alopecia secondary to superficial bacterial folliculitis




hemorrhagic bullae
Blood-filled elevation of epidermis, >1cm

Interdigital hemorrhagic bulla in a dog with deep pyoderma and furunculosis
comedo
dilated hair follicle filled with keratin, sebum
Comedones on the ventral abdomen of a dog with hypercortisolism
crust
Dried exudate and keratinous debris on skin surface

Multifocal crusts due to pemphigus foliaceus



epidermal collarettes
Circular scale or crust with erythema, associated with folliculitis or ruptured pustules or vesicles

Epidermal collarettes in a dog with Staphylococcus superficial bacterial folliculitis
erosion
Defect in epidermis that does not penetrate basement membrane. Histopathology may be needed to differentiate from ulcer.

Erosions in a dog with vasculitis
erythema
Red appearance of skin due to inflammation, capillary congestion

Erythema in a dog with cutaneous drug eruption
eschar
Thick crust often related to necrosis, trauma, or thermal/chemical burn

Eschar from physical trauma
excoriation
Erosions and/or ulcerations due to self-trauma

Excoriations in a cat with atopic dermatitis
fissure
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Fissures of the footpads in a dog with superficial necrolytic dermatitis
fistula
Ulcer on skin surface that originates from and is contiguous with tracts extending into deeper, typically subcutaneous tissues

Perianal fistulas in a dog
follicular casts
Accumulation of scale adherent to hair shaft

Follicular casts surrounding hairs from a dog with hypothyroidism
hyperkeratosis
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Idiopathic hyperkeratosis of the nasal planum (left) and footpads (right)
hyperpigmentation
Increased melanin in skin, often secondary to inflammation

Inflammatory lesions (left) resulting in post-inflammatory hyperpigmentation (right)

hypotrichosis
Lack of hair due to genetic factors or defects in embryogenesis.

Congenital hypotrichosis in chocolate Labrador puppies.

lichenification
Thickening of the epidermis, often due to chronic inflammation resulting in exaggerated texture

Lichenification of skin in a dog with chronic atopic dermatitis and Malassezia dermatitis
macule
Flat lesion associated with color change <1cm

Pigmented macule (left) Erythematous macule (right)
melanosis
Increased melanin in skin, may be secondary to inflammation.

Post inflammatory hyperpigmentation of this dog’s thigh
miliary
Multifocal, papular, crusting dermatitis; a descriptive term, not a diagnosis

Miliary dermatitis in a flea allergic cat
morbiliform
A erythematous, macular, papular rash; the erythematous macules are typically 2-10 mm in diameter with coalescence to form larger lesions in some areas

Morbiliform eruptions in a dog with a cutaneous drug reaction

onychodystrophy
Abnormal nail morphology due to nail bed infection, inflammation, or trauma; may include: Onychogryphosis, Onychomadesis, Onychorrhexis, Onychoschizia

Onychodystrophy in dog with chronic allergies
onychogryphosis
Abnormal claw curvature; secondary to nail bed inflammation or trauma

Onychogryphosis in a dog with symmetric lupoid onychodystrophy
onychomadesis
Claw sloughing due to nail bed inflammation or trauma

Onychomadesis in a dog with symmetric lupoid onychodystrophy
onychorrhexis
Claw fragmentation due to nail bed inflammation or trauma

Onychorrhexis in a dog with symmetric lupoid onychodystrophy
onychoschizia
Claw splitting due to nail bed inflammation or trauma

Onychoschizia in a dog with symmetric lupoid onychodystrophy

patch
Flat lesion associated with color change >1cm

Hypopigmented patch (left), erythematous patch (right)
petechiae
Small erythematous or violaceous lesions due to dermal bleeding

Petechiae in a dog with cutaneous vasculitis
phlebectasia
Venous dilation; most commonly associated with hypercortisolism

Phlebectasia and cutaneous atrophy due to hypercortisolism in a dog
plaques
Flat-topped elevation >1cm formed of coalescing papules or dermal infiltration

Plaques in a cat with cutaneous lymphoma
pustule
Raised epidermal infiltration of pus

Pustules on the abdomen of a dog with superficial staphylococcal pyoderma.
scale
Accumulation of loose fragments of stratum corneum

Loose, large scales due to ichthyosis in a Golden Retriever
scar
Fibrous tissue replacing damaged cutaneous and/or subcutaneous tissues

Scarring (right) following the healing of an ulcer (left) in a dog with sterile nodular dermatitis
serpiginous
Undulating, serpentine (snake-like) arrangement of lesions

Serpiginous urticarial lesions on a horse
telangiectasia
Permanent enlargement of vessels resulting in a red or violet lesion (rare)

Telangiectasia in a dog with angiomatosis
ulcer
A defect in epidermis that penetrates the basement membrane. Histopathology may be needed to differentiate from an erosion.

Ulcerations of the skin of a dog with vasculitis.
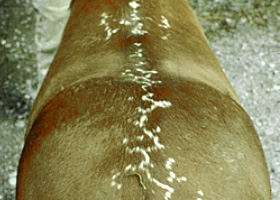
urticaria
Wheals (steep-walled, circumscribed elevation in the skin due to edema ) due to hypersensitivity reaction

Urticaria in a horse
vesicle
Fluid-filled elevation of epidermis, <1cm

Vesicles and bullae on ear pinna due to bullous pemphigoid
wheal
Steep-walled, circumscribed elevation in the skin due to edema
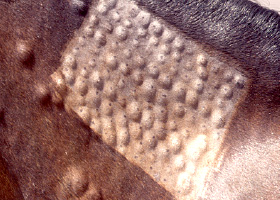
Wheals associated with intradermal allergy testing in a horse