CUTANEOUS CYTOLOGY
When do I do it?
- When bacterial or yeast infection is suspected (inflammatory alopecia, seborrhea, scales, papule, pustule, crust, erosions, ulcer)
- In patients with nodule/tumors- do cytology on every nodule/tumor
- In patients with suspected pemphigoid diseases (erosions, pustule, crust)
- In every patient with otitis externa
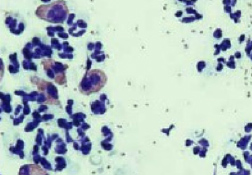
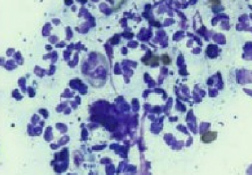
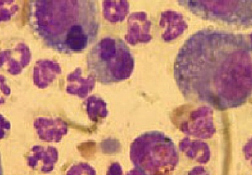
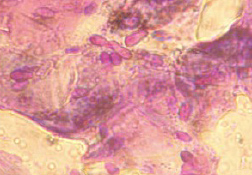
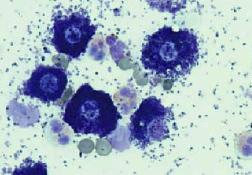
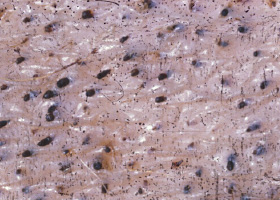
What can I find?
- Cocci (most likely Staphylococcus sp.)
- Rods → culture and susceptibility advisable
- Inflammatory cells with intracellular bacteria → clinically relevant infection that may require systemic antibiotic treatment
- Eosinophils → can point to ectoparasites or allergies
- Macrophages → seen in chronic, sterile and infectious processes
- Malassezia spp. → one or more Malassezia sp. per oil immersion field (x 1000 magnification) may be clinically relevant (normal numbers vary can vary with the climate.) In cases of Malassezia hypersensitivity a much lower number of Malassezia (e.g. one in every two or three HPFs) can cause clinical disease. Topical or systemic treatment should be considered.
- Neoplastic cells




What do I need?
- Slides, DiffQuick® or similar stain, mineral oil, adhesive tape, microscope, needle and syringe
How do I do it?
- Rub or impress a slide on moist, exuding or greasy surface of infected skin.
- Role a cotton bud on the skin surface or insert it in the ears and role cotton bud on the slide.
- Insert needle (25 - 27 ga.) into the pustule holding the needle parallel to the skin so that only the pustule is punctured, no deeper cells or blood are required, top is lifted off and slide impressed onto the ruptured pustule.
- Use the sticky surface of the adhesive tape to collect cells and surface organisms from dry and / or scaly skin and then place this (sticky side down) onto a glass slide with a drop of the blue Difff-Quick® stain. The tape acts as its own coverslip.
- Apply a piece of double-sided adhesive tape to a slide and collect material with the sticky slide. Stain this in the blue Diff-Quick® stain, dry and examine under oil immersion.
- Insert needle into nodule or abscesses and re-insert a number of times without leaving the skin. Withdraw the needle. A syringe with the plunger pulled back is attached to the needle and contents is blown onto a slide and air dried.
- Stain the air dried slides (e.g. Diff-Quick®)
- Put the slides under a microscope, condenser up.
Tip
- Moisten a cotton bud with saline solution or carefully rub the edge of a slide on the skin and then rub the material on the slide
- Press clear adhesive tape (sticky side down) onto the skin. Stain the tape like a slide, let it air dry and press it onto a slide or put a drop of the blue stain o DiffQuick® on a slide and press the tape sticky side down on the drop. Evaluate under a microscope.



abscess
A discrete swelling containing purulent material, typically in the subcutis

Perianal abscess in a dog
alopecia
Absence of hair from areas where it is normally present; may be due to folliculitis, abnormal follicle cycling, or self-trauma

Extensive alopecia secondary to cutaneous epitheliotropic lymphoma
alopecia (“moth-eaten”)
well-circumscribed, circular, patchy to coalescing alopecia, often associated with folliculitis

“Moth-eaten” alopecia secondary to superficial bacterial folliculitis




hemorrhagic bullae
Blood-filled elevation of epidermis, >1cm

Interdigital hemorrhagic bulla in a dog with deep pyoderma and furunculosis
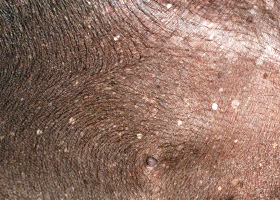
comedo
dilated hair follicle filled with keratin, sebum
Comedones on the ventral abdomen of a dog with hypercortisolism
crust
Dried exudate and keratinous debris on skin surface

Multifocal crusts due to pemphigus foliaceus



epidermal collarettes
Circular scale or crust with erythema, associated with folliculitis or ruptured pustules or vesicles

Epidermal collarettes in a dog with Staphylococcus superficial bacterial folliculitis
erosion
Defect in epidermis that does not penetrate basement membrane. Histopathology may be needed to differentiate from ulcer.

Erosions in a dog with vasculitis
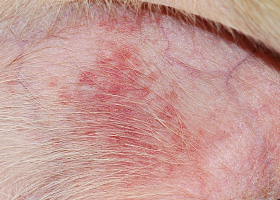
erythema
Red appearance of skin due to inflammation, capillary congestion

Erythema in a dog with cutaneous drug eruption
eschar
Thick crust often related to necrosis, trauma, or thermal/chemical burn

Eschar from physical trauma
excoriation
Erosions and/or ulcerations due to self-trauma

Excoriations in a cat with atopic dermatitis
fissure
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Fissures of the footpads in a dog with superficial necrolytic dermatitis
fistula
Ulcer on skin surface that originates from and is contiguous with tracts extending into deeper, typically subcutaneous tissues

Perianal fistulas in a dog
follicular casts
Accumulation of scale adherent to hair shaft

Follicular casts surrounding hairs from a dog with hypothyroidism
hyperkeratosis
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Idiopathic hyperkeratosis of the nasal planum (left) and footpads (right)
hyperpigmentation
Increased melanin in skin, often secondary to inflammation

Inflammatory lesions (left) resulting in post-inflammatory hyperpigmentation (right)

hypotrichosis
Lack of hair due to genetic factors or defects in embryogenesis.

Congenital hypotrichosis in chocolate Labrador puppies.

lichenification
Thickening of the epidermis, often due to chronic inflammation resulting in exaggerated texture

Lichenification of skin in a dog with chronic atopic dermatitis and Malassezia dermatitis
macule
Flat lesion associated with color change <1cm

Pigmented macule (left) Erythematous macule (right)
melanosis
Increased melanin in skin, may be secondary to inflammation.

Post inflammatory hyperpigmentation of this dog’s thigh
miliary
Multifocal, papular, crusting dermatitis; a descriptive term, not a diagnosis

Miliary dermatitis in a flea allergic cat
morbiliform
A erythematous, macular, papular rash; the erythematous macules are typically 2-10 mm in diameter with coalescence to form larger lesions in some areas

Morbiliform eruptions in a dog with a cutaneous drug reaction

onychodystrophy
Abnormal nail morphology due to nail bed infection, inflammation, or trauma; may include: Onychogryphosis, Onychomadesis, Onychorrhexis, Onychoschizia

Onychodystrophy in dog with chronic allergies
onychogryphosis
Abnormal claw curvature; secondary to nail bed inflammation or trauma

Onychogryphosis in a dog with symmetric lupoid onychodystrophy
onychomadesis
Claw sloughing due to nail bed inflammation or trauma

Onychomadesis in a dog with symmetric lupoid onychodystrophy
onychorrhexis
Claw fragmentation due to nail bed inflammation or trauma

Onychorrhexis in a dog with symmetric lupoid onychodystrophy
onychoschizia
Claw splitting due to nail bed inflammation or trauma

Onychoschizia in a dog with symmetric lupoid onychodystrophy

patch
Flat lesion associated with color change >1cm

Hypopigmented patch (left), erythematous patch (right)
petechiae
Small erythematous or violaceous lesions due to dermal bleeding

Petechiae in a dog with cutaneous vasculitis
phlebectasia
Venous dilation; most commonly associated with hypercortisolism

Phlebectasia and cutaneous atrophy due to hypercortisolism in a dog
plaques
Flat-topped elevation >1cm formed of coalescing papules or dermal infiltration

Plaques in a cat with cutaneous lymphoma
pustule
Raised epidermal infiltration of pus

Pustules on the abdomen of a dog with superficial staphylococcal pyoderma.
scale
Accumulation of loose fragments of stratum corneum

Loose, large scales due to ichthyosis in a Golden Retriever
scar
Fibrous tissue replacing damaged cutaneous and/or subcutaneous tissues

Scarring (right) following the healing of an ulcer (left) in a dog with sterile nodular dermatitis
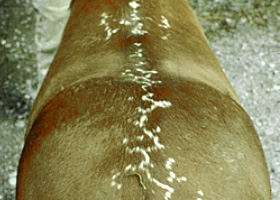
serpiginous
Undulating, serpentine (snake-like) arrangement of lesions

Serpiginous urticarial lesions on a horse
telangiectasia
Permanent enlargement of vessels resulting in a red or violet lesion (rare)

Telangiectasia in a dog with angiomatosis
ulcer
A defect in epidermis that penetrates the basement membrane. Histopathology may be needed to differentiate from an erosion.

Ulcerations of the skin of a dog with vasculitis.
urticaria
Wheals (steep-walled, circumscribed elevation in the skin due to edema ) due to hypersensitivity reaction

Urticaria in a horse
vesicle
Fluid-filled elevation of epidermis, <1cm

Vesicles and bullae on ear pinna due to bullous pemphigoid
wheal
Steep-walled, circumscribed elevation in the skin due to edema
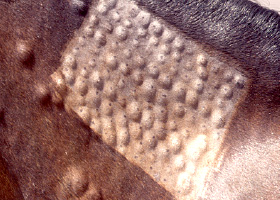
Wheals associated with intradermal allergy testing in a horse