Fungal & Yeast Dermatoses : MALASSEZIA DERMATITIS
- At a glance
- WHAT DOES IT LOOK LIKE?
- WHAT ELSE LOOKS LIKE THIS?
- HOW DO I DIAGNOSE IT?
- HOW DO I MANAGE IT?
- COMMENTS
AT A GLANCE
- A superficial epidermal overgrowth of the commensal yeast, Malassezia pachydermatis.
- A common diagnosis in dogs, uncommon in cats, but possibly under diagnosed in this species.
- Other species in the genus Malassezia are recognized commensals of dogs and cats, but appear to be much less frequently involved in dermatitis.
- Malassezia dermatitis develops secondarily to allergic, endocrine, conformational, and keratinization disorders and rarely develops due to immunocompromised status.
- Increased warmth and humidity of the environment and protected cutaneous microenvironments, such as skin folds and ear canals, appear to be predisposing factors for Malassezia colonization.
- Malassezia is not an invasive organism and remains confined to the stratum corneum. Enzymes produced by Malassezia stimulate pruritus and inflammatory changes.
- Hypersensitivity to Malassezia is considered to be a significant potential contributor to pruritus and may occur more frequently in dogs and cats with atopic dermatitis, as it does in atopic humans.
- Concurrent overgrowth of Staphylococcus species is common.
- Basset hounds, West Highland white terriers, and American cocker spaniels are over-represented, as well as Devon rex and sphinx cats.










WHAT DOES IT LOOK LIKE?
- Clinical signs are non-specific and may include:
- Pruritus
- Malodor
- Erythema
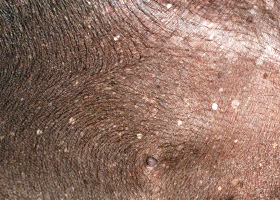
- Scale
- Greasy or waxy skin debris
- Lesions consistent with self-trauma due to pruritus
- Hyperpigmentation and lichenification
- Rust or brown pigmentation of hair or proximal claw (with claw fold involvement)
- Feline chin acne
- Common locations include:
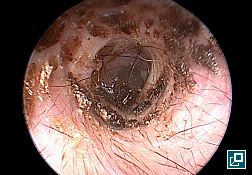
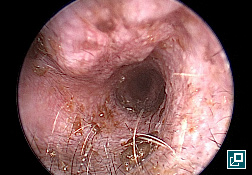
- Ear canals
- Lip margins and lip folds
- Axilla
- Groin
- Ventral neck
- Perineum
- Interdigital spaces and claw folds
- Skin folds (e.g., facial folds of English bulldogs and others)
- Importantly, Staphylococcus infections, and associated lesions, are often concurrently present.
WHAT ELSE LOOKS LIKE THIS?
- Staphylococcal pyoderma
- Demodicosis
- Dermatophytosis
- Cheyletiellosis
- Sarcoptic mange
- Canine hypothyroidism
- Hypersensitivity syndromes: flea-bite hypersensitivity, cutaneous adverse food reaction, atopic dermatitis and contact hypersensitivity
- Primary keratinization disorders
- Epitheliotropic cutaneous lymphoma
HOW DO I DIAGNOSE IT?
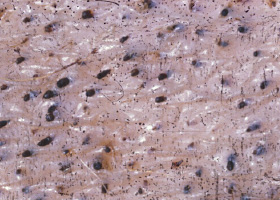
- Diagnosis is confirmed via cutaneous cytology.
- Although malodor is a common feature, its presence or absence may be misleading. Cytological evaluation is strongly recommended.
- Numbers of Malassezia organisms are variable.
- A finding of greater than 3 yeasts per high power oil immersion field is significant in the presence of suggestive clinical signs.
- Clinical signs may be present with fewer numbers of yeast in some individuals.
- Positive reactions to intradermally-injected Malassezia antigen or elevated levels of Malassezia-specific IgE support the diagnosis of Malassezia hypersensitivity in pruritic patients with Malassezia overgrowth. These diagnostics are not routinely performed and not required for diagnosis.
HOW DO I MANAGE IT?
- Treatment involves management of the underlying condition as well as topical and/or systemic antifungal therapy.
- Recheck with repeat cytology should be performed 1-3 weeks after initiation of therapy and approximately one week beyond clinical and cytological cure.
- The typical treatment duration is 3-4 weeks.
- Topical therapy is indicated in all cases of Malassezia dermatitis and should be utilized in conjunction with systemic therapy for generalized presentations.
- Shampoo therapy is ideally performed 2-3 times weekly. Shampoos should be continued until resolution, and can be maintained weekly to prevent recurrence. A minimum of 10 minutes is a suggested contact time.
- Effective active ingredients include: ketoconazole 1-2%, miconazole 2%, chlorhexidine 2-4%, benzoyl peroxide 2.5%, and selenium sulfide 1%.
- Sprays and wipes containing acetic acid 2% and boric acid 2%, chlorhexidine 2-4%, miconazole 2%, or ketoconazole 1-2% may be used every 24-48 hours until resolution, and can be maintained 1-2 times weekly to prevent recurrence.
- Leave-on rinses with the following active ingredients may be utilized as a sole or adjunct topical treatment: acetic acid 2%, ketoconazole 1-2% miconazole 2%, and chlorhexidine 2-4%. A white vinegar and water (1:3) solution may be utilized as an acetic acid leave-on rinse.
- Focal, dry presentations may be treated with daily applications of antifungal lotions, ointment, or creams.
- Active ingredients include: clotrimazole 1%, miconazole 1-2%, terbinafine 1%, thiabendazole 4%, amphotericin B 3% and nystatin.
- Systemic antifungal treatment is recommended for patients with generalized or multifocal Malassezia colonization and can be used as a sole therapy when compliance with topical therapy is poor.
- Systemic therapy is selected empirically. Culture and sensitivity of Malassezia is not routinely performed by laboratories, and reliable, reproducible susceptibility breakpoints are yet to be established and correlated with clinical efficacy.
- The typical treatment duration is 3-4 weeks. Recheck is recommended to assess for clinical and cytological response.
| MEDICATION | DOSE |
|---|---|
| Ketoconazole |
5-10 mg/kg PO q 24 hours |
| Itraconazole |
5-10 mg/kg PO q 24 hours or 2 consecutive days per week |
| Fluconazole |
10 mg/kg PO q 24 hours |
| Terbinafine |
30 mg/kg PO q 24 hours or 2 consecutive days per week |
- Ketoconazole and itraconazole should be given with food to optimize absorption.
- The azole class of antifungals may induce hepatotoxicity and should be avoided or used with caution in patients with hepatotoxicity. Many drug interactions with this class are possible and concurrent medications should be assessed. For prolonged use of the azole class antifungals, a serum biochemistry profile is prudent to assess for hepatotoxicity.
- Vasculitis and cutaneous ulcer may develop in 7.5% of dogs treated with itraconazole at doses ≥10 mg/kg.
- Malassezia antigens may be included in immunotherapy preparations for patients with treatment of atopic dermatitis. At present evidence for efficacy of immunotherapy in patients with suspected Malassezia hypersensitivity is lacking.
COMMENTS
- The most common causes of treatment failure are inadequate treatment duration and failure to control underlying dermatologic disease.
- For patients with atopic dermatitis, topical maintenance therapy, particularly in folds and interdigital spaces, is helpful to prevent relapse and to treat associated pruritus.
- Malassezia with in vitro resistance to ketoconazole, fluconazole, and intraconazole has been documented. However, in vivo resistance has not been well-documented.
References
- Foy DS, Trepanier LA. Antifungal Treatment of Small Animal Veterinary Patients. Vet Clin North Am Small Anim Pract. 2010; 40: 1171-88
- Nuttall T. Harvey G. McKeever. PJ. Skin Diseases of the Dog and Cat. 2009.59.
abscess
A discrete swelling containing purulent material, typically in the subcutis

Perianal abscess in a dog
alopecia
Absence of hair from areas where it is normally present; may be due to folliculitis, abnormal follicle cycling, or self-trauma

Extensive alopecia secondary to cutaneous epitheliotropic lymphoma
alopecia (“moth-eaten”)
well-circumscribed, circular, patchy to coalescing alopecia, often associated with folliculitis

“Moth-eaten” alopecia secondary to superficial bacterial folliculitis




hemorrhagic bullae
Blood-filled elevation of epidermis, >1cm

Interdigital hemorrhagic bulla in a dog with deep pyoderma and furunculosis
comedo
dilated hair follicle filled with keratin, sebum
Comedones on the ventral abdomen of a dog with hypercortisolism
crust
Dried exudate and keratinous debris on skin surface

Multifocal crusts due to pemphigus foliaceus



epidermal collarettes
Circular scale or crust with erythema, associated with folliculitis or ruptured pustules or vesicles

Epidermal collarettes in a dog with Staphylococcus superficial bacterial folliculitis
erosion
Defect in epidermis that does not penetrate basement membrane. Histopathology may be needed to differentiate from ulcer.

Erosions in a dog with vasculitis
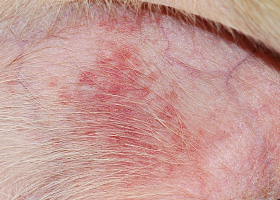
erythema
Red appearance of skin due to inflammation, capillary congestion

Erythema in a dog with cutaneous drug eruption
eschar
Thick crust often related to necrosis, trauma, or thermal/chemical burn

Eschar from physical trauma
excoriation
Erosions and/or ulcerations due to self-trauma

Excoriations in a cat with atopic dermatitis
fissure
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Fissures of the footpads in a dog with superficial necrolytic dermatitis
fistula
Ulcer on skin surface that originates from and is contiguous with tracts extending into deeper, typically subcutaneous tissues

Perianal fistulas in a dog
follicular casts
Accumulation of scale adherent to hair shaft

Follicular casts surrounding hairs from a dog with hypothyroidism
hyperkeratosis
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Idiopathic hyperkeratosis of the nasal planum (left) and footpads (right)
hyperpigmentation
Increased melanin in skin, often secondary to inflammation

Inflammatory lesions (left) resulting in post-inflammatory hyperpigmentation (right)

hypotrichosis
Lack of hair due to genetic factors or defects in embryogenesis.

Congenital hypotrichosis in chocolate Labrador puppies.

lichenification
Thickening of the epidermis, often due to chronic inflammation resulting in exaggerated texture

Lichenification of skin in a dog with chronic atopic dermatitis and Malassezia dermatitis
macule
Flat lesion associated with color change <1cm

Pigmented macule (left) Erythematous macule (right)
melanosis
Increased melanin in skin, may be secondary to inflammation.

Post inflammatory hyperpigmentation of this dog’s thigh
miliary
Multifocal, papular, crusting dermatitis; a descriptive term, not a diagnosis

Miliary dermatitis in a flea allergic cat
morbiliform
A erythematous, macular, papular rash; the erythematous macules are typically 2-10 mm in diameter with coalescence to form larger lesions in some areas

Morbiliform eruptions in a dog with a cutaneous drug reaction

onychodystrophy
Abnormal nail morphology due to nail bed infection, inflammation, or trauma; may include: Onychogryphosis, Onychomadesis, Onychorrhexis, Onychoschizia

Onychodystrophy in dog with chronic allergies
onychogryphosis
Abnormal claw curvature; secondary to nail bed inflammation or trauma

Onychogryphosis in a dog with symmetric lupoid onychodystrophy
onychomadesis
Claw sloughing due to nail bed inflammation or trauma

Onychomadesis in a dog with symmetric lupoid onychodystrophy
onychorrhexis
Claw fragmentation due to nail bed inflammation or trauma

Onychorrhexis in a dog with symmetric lupoid onychodystrophy
onychoschizia
Claw splitting due to nail bed inflammation or trauma

Onychoschizia in a dog with symmetric lupoid onychodystrophy

patch
Flat lesion associated with color change >1cm

Hypopigmented patch (left), erythematous patch (right)
petechiae
Small erythematous or violaceous lesions due to dermal bleeding

Petechiae in a dog with cutaneous vasculitis
phlebectasia
Venous dilation; most commonly associated with hypercortisolism

Phlebectasia and cutaneous atrophy due to hypercortisolism in a dog
plaques
Flat-topped elevation >1cm formed of coalescing papules or dermal infiltration

Plaques in a cat with cutaneous lymphoma
pustule
Raised epidermal infiltration of pus

Pustules on the abdomen of a dog with superficial staphylococcal pyoderma.
scale
Accumulation of loose fragments of stratum corneum

Loose, large scales due to ichthyosis in a Golden Retriever
scar
Fibrous tissue replacing damaged cutaneous and/or subcutaneous tissues

Scarring (right) following the healing of an ulcer (left) in a dog with sterile nodular dermatitis
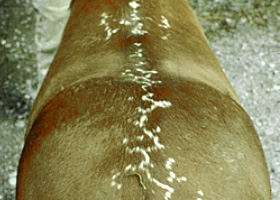
serpiginous
Undulating, serpentine (snake-like) arrangement of lesions

Serpiginous urticarial lesions on a horse
telangiectasia
Permanent enlargement of vessels resulting in a red or violet lesion (rare)

Telangiectasia in a dog with angiomatosis
ulcer
A defect in epidermis that penetrates the basement membrane. Histopathology may be needed to differentiate from an erosion.

Ulcerations of the skin of a dog with vasculitis.
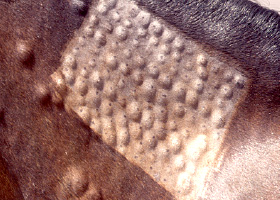
urticaria
Wheals (steep-walled, circumscribed elevation in the skin due to edema ) due to hypersensitivity reaction

Urticaria in a horse
vesicle
Fluid-filled elevation of epidermis, <1cm

Vesicles and bullae on ear pinna due to bullous pemphigoid
wheal
Steep-walled, circumscribed elevation in the skin due to edema
Wheals associated with intradermal allergy testing in a horse