PARASITIC DERMATOSES : SARCOPTIC MANGE (CANINE SCABIES)
- At a glance
- WHAT DOES IT LOOK LIKE?
- WHAT ELSE LOOKS LIKE THIS?
- HOW DO I DIAGNOSE IT?
- HOW DO I MANAGE IT?
- COMMENTS
AT A GLANCE
- Non-seasonal, intensely pruritic, highly contagious infestation of the skin of dogs caused by the mite Sarcoptes scabiei var. canis
- Zoonotic






WHAT DOES IT LOOK LIKE?
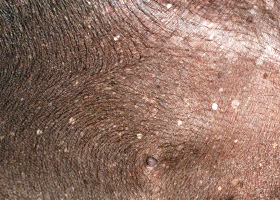
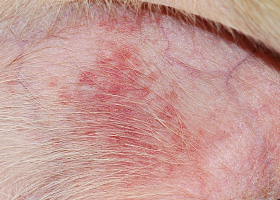
- Pinnal margins, face, abdomen, chest, elbows, hocks, feet
- Pruritic papule, crusted papule, alopecia, erythema
- Chronic infestation leads to thick yellow crust, hyperpigmentation and lichenification of the skin and peripheral lymphadenopathy
WHAT ELSE LOOKS LIKE THIS?
- Allergic dermatitis (contact, atopic dermatitis, cutaneous adverse reaction to food (CARF))
- Malassezia dermatitis
- Cheyletiellosis
- Otodectic dermatitis
- Pelodera dermatitis
HOW DO I DIAGNOSE IT?
- Pinnal-pedal reflex elicited (non-specific; positive in 50-90% cases)
- Superficial skin scrapings:
- Multiple sites
- Higher yield in non-excoriated skin of ear margins, elbows, hocks and in crust
- Mite, mite parts, eggs or feces is diagnostic (positive in 20-50% of cases)
- Prophylactic treatment trial
- Histopathology (rarely conclusive)
HOW DO I MANAGE IT?
- Start treatment as soon as diagnosis is made or suspected
- Treatment can be either topical or systemic, and should include all dogs in contact (including asymptomatic carriers)
Hair can be clipped (medium to long-hair), the crust and dirt removed by soaking with an antiseborrheic shampoo, and an acaricidal dip applied.
- Lime sulfur is highly effective and safe for use in young animals; weekly 2-4% lime sulfur dips for 4-6 treatments are recommended.
- Organophosphate dips can be effective
- Selamectin spot-on formulation is approved for scabies treatment.
- Studies show cure with labeled indication of 2 doses at 30-day intervals. 5% of dogs have been shown to harbor live mites at day 30 with 100% cure rate at day 60.
- Imidacloprid/moxidectin spot-on formulation is labeled for scabies treatment in Canada and is available in the Canada. Studies show two doses applied at 30-day intervals are 100% effective after 60 days.
- Ivermectin can be given off-label at dosages of 0.2-0.4 mg/kg by mouth once weekly at 7-day intervals for 3 treatments or 0.2mg/kg by subcutaneous injection every two weeks for 2 treatments. At this dosage, the drug is contraindicated in dogs with multiple drug-resistant gene ABCB1 (formerly MDR1) mutation. Idiosyncratic reactions in other breeds may also occur.
- Prior to treatment with macrocyclic lactone/ avermectins, dogs should be heartworm test negative and evaluated for possible neurotoxicity by test dosing or determination of ABCB1- delta1 (MDR-1) gene status.
Note toxicity has occurred in dogs with normal ABCB1- delta1 gene function, therefore recommend test dosing by starting with 0.05 mg/kg by mouth daily and gradually increasing to the target dose, the owner should be instructed to stop administration if the animal exhibits mydriasis, hypersalivation, depression, ataxia or any other side effects. - For more information: Washington State University, College of Veterinary Medicine, Clinical Pathology Laboratory (www.vetmed.wsu.edu/deptsclinpath/index.aspx)
- DO NOT USE SPINOSAD concurrently with high dose, increased frequency macrocyclic lactone/ avermectin therapy.
- Prior to treatment with macrocyclic lactone/ avermectins, dogs should be heartworm test negative and evaluated for possible neurotoxicity by test dosing or determination of ABCB1- delta1 (MDR-1) gene status.
- Markedly pruritic dogs can benefit from treatment with glucocorticoids for 5-7 days.
- Secondary bacterial infections should be treated appropriately.
COMMENTS
- Scabies mites can live in the environment for up to 21 days.
- Cleaning and applying an environmental pesticide may be indicated in severe cases or in multiple pet households.
- If lesions are present on in-contact humans, they may persist for 7-14 days, but new lesions should not develop. Development of new lesions indicates inadequate treatment of the dogs, environmental infestation, or true human scabies, which could have been transferred to the dogs. The owners should be referred to a human dermatologist.
- Wild carnivores including foxes and coyotes are common sources of infestation.
- Miller W, Griffin C, Campbell K. Muller and Kirk's Small Animal Dermatology, ed 7, Philadelphia: Elsevier, 2013, pp 315-319.
- The Merck Veterinary Manual. Sarcoptic Mange (Canine Scabies). Available at: www.merckvetmanual.com/mvm/index.jsp?cfile=htm/bc/72005.htm. Accessed February 1, 2013.
abscess
A discrete swelling containing purulent material, typically in the subcutis

Perianal abscess in a dog
alopecia
Absence of hair from areas where it is normally present; may be due to folliculitis, abnormal follicle cycling, or self-trauma

Extensive alopecia secondary to cutaneous epitheliotropic lymphoma
alopecia (“moth-eaten”)
well-circumscribed, circular, patchy to coalescing alopecia, often associated with folliculitis

“Moth-eaten” alopecia secondary to superficial bacterial folliculitis




hemorrhagic bullae
Blood-filled elevation of epidermis, >1cm

Interdigital hemorrhagic bulla in a dog with deep pyoderma and furunculosis
comedo
dilated hair follicle filled with keratin, sebum
Comedones on the ventral abdomen of a dog with hypercortisolism
crust
Dried exudate and keratinous debris on skin surface

Multifocal crusts due to pemphigus foliaceus



epidermal collarettes
Circular scale or crust with erythema, associated with folliculitis or ruptured pustules or vesicles

Epidermal collarettes in a dog with Staphylococcus superficial bacterial folliculitis
erosion
Defect in epidermis that does not penetrate basement membrane. Histopathology may be needed to differentiate from ulcer.

Erosions in a dog with vasculitis
erythema
Red appearance of skin due to inflammation, capillary congestion

Erythema in a dog with cutaneous drug eruption
eschar
Thick crust often related to necrosis, trauma, or thermal/chemical burn

Eschar from physical trauma
excoriation
Erosions and/or ulcerations due to self-trauma

Excoriations in a cat with atopic dermatitis
fissure
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Fissures of the footpads in a dog with superficial necrolytic dermatitis
fistula
Ulcer on skin surface that originates from and is contiguous with tracts extending into deeper, typically subcutaneous tissues

Perianal fistulas in a dog
follicular casts
Accumulation of scale adherent to hair shaft

Follicular casts surrounding hairs from a dog with hypothyroidism
hyperkeratosis
Excessive stratum corneum, confirmed via histopathology. This term is often used to describe the nasal planum and footpads.

Idiopathic hyperkeratosis of the nasal planum (left) and footpads (right)
hyperpigmentation
Increased melanin in skin, often secondary to inflammation

Inflammatory lesions (left) resulting in post-inflammatory hyperpigmentation (right)

hypotrichosis
Lack of hair due to genetic factors or defects in embryogenesis.

Congenital hypotrichosis in chocolate Labrador puppies.

lichenification
Thickening of the epidermis, often due to chronic inflammation resulting in exaggerated texture

Lichenification of skin in a dog with chronic atopic dermatitis and Malassezia dermatitis
macule
Flat lesion associated with color change <1cm

Pigmented macule (left) Erythematous macule (right)
melanosis
Increased melanin in skin, may be secondary to inflammation.

Post inflammatory hyperpigmentation of this dog’s thigh
miliary
Multifocal, papular, crusting dermatitis; a descriptive term, not a diagnosis

Miliary dermatitis in a flea allergic cat
morbiliform
A erythematous, macular, papular rash; the erythematous macules are typically 2-10 mm in diameter with coalescence to form larger lesions in some areas

Morbiliform eruptions in a dog with a cutaneous drug reaction

onychodystrophy
Abnormal nail morphology due to nail bed infection, inflammation, or trauma; may include: Onychogryphosis, Onychomadesis, Onychorrhexis, Onychoschizia

Onychodystrophy in dog with chronic allergies
onychogryphosis
Abnormal claw curvature; secondary to nail bed inflammation or trauma

Onychogryphosis in a dog with symmetric lupoid onychodystrophy
onychomadesis
Claw sloughing due to nail bed inflammation or trauma

Onychomadesis in a dog with symmetric lupoid onychodystrophy
onychorrhexis
Claw fragmentation due to nail bed inflammation or trauma

Onychorrhexis in a dog with symmetric lupoid onychodystrophy
onychoschizia
Claw splitting due to nail bed inflammation or trauma

Onychoschizia in a dog with symmetric lupoid onychodystrophy

patch
Flat lesion associated with color change >1cm

Hypopigmented patch (left), erythematous patch (right)
petechiae
Small erythematous or violaceous lesions due to dermal bleeding

Petechiae in a dog with cutaneous vasculitis
phlebectasia
Venous dilation; most commonly associated with hypercortisolism

Phlebectasia and cutaneous atrophy due to hypercortisolism in a dog
plaques
Flat-topped elevation >1cm formed of coalescing papules or dermal infiltration

Plaques in a cat with cutaneous lymphoma
pustule
Raised epidermal infiltration of pus

Pustules on the abdomen of a dog with superficial staphylococcal pyoderma.
scale
Accumulation of loose fragments of stratum corneum

Loose, large scales due to ichthyosis in a Golden Retriever
scar
Fibrous tissue replacing damaged cutaneous and/or subcutaneous tissues

Scarring (right) following the healing of an ulcer (left) in a dog with sterile nodular dermatitis
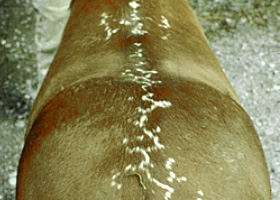
serpiginous
Undulating, serpentine (snake-like) arrangement of lesions

Serpiginous urticarial lesions on a horse
telangiectasia
Permanent enlargement of vessels resulting in a red or violet lesion (rare)

Telangiectasia in a dog with angiomatosis
ulcer
A defect in epidermis that penetrates the basement membrane. Histopathology may be needed to differentiate from an erosion.

Ulcerations of the skin of a dog with vasculitis.
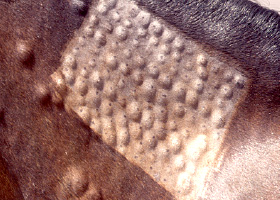
urticaria
Wheals (steep-walled, circumscribed elevation in the skin due to edema ) due to hypersensitivity reaction

Urticaria in a horse
vesicle
Fluid-filled elevation of epidermis, <1cm

Vesicles and bullae on ear pinna due to bullous pemphigoid
wheal
Steep-walled, circumscribed elevation in the skin due to edema
Wheals associated with intradermal allergy testing in a horse